Volume 3, Issue 8
August 2023
A Pediatric Monteggia Fracture Unattended for Five Years
Meshal Yahya Altowairqi, Mohammad Mofareh Alsubaie, Oqab Muidh Almalki
DOI: http://dx.doi.org/10.52533/JOHS.2023.30805
Keywords: neglected, Monteggia, fracture, radial
Background: The Monteggia fracture classically involves a proximal third ulna fracture that is accompanied by radial head subluxation or dislocation. Monteggia fractures are highly uncommon, as they account for just 1% of pediatric forearm fractures. However, Monteggia fractures continue to be a concern for pediatric orthopedic surgeons due to the difficulties in diagnosing and treating missing radial head dislocations and late instability.
Case: We report the case of a 14-year-old boy who suffered from a neglected Monteggia fracture that was missed for five long years. The patient reported to the clinic with limited range of motion and elbow pain during activities. No neurological or other significant complications were observed. X-ray and Computed Tomography (CT) scan findings confirmed the diagnosis of a neglected Monteggia fracture. The patient was managed through rehabilitation involving physiotherapy sessions since the parents refused surgical intervention.
Conclusion: Our case is unique to the present since it is the only case, to the best of our knowledge, with such an increased time duration of neglected Monteggia fracture, and additionally, it was managed with rehabilitation only. However, further research is necessary to study more alternative management options for the management of neglected Monteggia fractures.
Introduction
A Monteggia fracture classically involves a proximal third ulna fracture that is accompanied by radial head subluxation or dislocation. Monteggia fractures are highly uncommon, as they account for just 1% of pediatric forearm fractures. Nevertheless, they are a significant fracture to recognize as almost all of them call for immediate orthopedic intervention, and a delayed diagnosis or missed fracture may result in poor long-term outcomes, such as chronic valgus instability and radiocapitellar osteoarthrosis, while an anteriorly dislocated radial head may result in impingement that results in radial neuropathy. Additionally, the radial head becomes irreducible after a period of two to three weeks (1).
Monteggia fractures are classified into four types by Bado. Type 1 includes an ulna shaft fracture along with an anterior radial head dislocation, while type 2 refers to an ulna shaft fracture alongside a posterior radial head dislocation. Type 3 involves an ulna shaft fracture together with an anterior lateral head dislocation, and type 4 is an ulna shaft fracture combined with a fracture of the radius and dislocation in any direction. Plastic deformation of the ulna without fracture and radial head dislocation are pediatric variations of this fracture (2, 3). A neglected Monteggia fracture is described as a proximal ulna fracture associated with radial head dislocation that has not been treated for 4 weeks or longer after injury. The natural course of chronic Monteggia lesions is unknown, but some patients experience pain, loss of motion, particularly in flexion and supination, elbow deformity, and even arthritis (4).
Monteggia fractures continue to be a concern for pediatric orthopedic surgeons due to the difficulties in diagnosing and treating missing radial head dislocations and late instability. The aim of treatment is to stabilize the ulnar fracture and radial head dislocation. The ulnar fracture deformity is reduced with a mix of longitudinal traction, elbow rotation, and manual manipulation; after the ulnar length is restored, the radiocapitellar joint will often diminish naturally or as a result of pressure on the radial head. The purpose of treatment algorithms based on the ulnar fracture pattern is to minimize complications and maximize outcomes by restoring and maintaining ulnar alignment (5). We report a case of Monteggia fracture that remained neglected for five long years.
Case Presentation
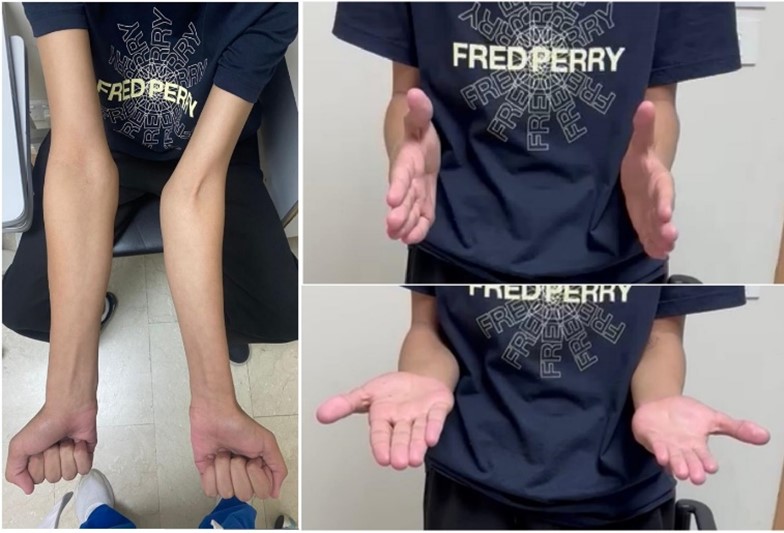
A fourteen-year-old male with no significant past medical history presented to the orthopedic clinic with a complaint of mild left elbow pain during weight-bearing activities and slightly less arc/range of motion in comparison to the contralateral side. The patient reported that he suffered from an ulnar shaft fracture five years ago, which was treated non-operatively. During that time, the radial head anterior dislocation was missed, and the patient lost follow-up in the clinic. The physical examination showed a left elbow extension lag of 30 degrees, flexion to 130 degrees, supination and pronation were full without limitation or pain, and he had no tenderness with palpation over the elbow. Furthermore, no motor or sensory deficits were noted or observed (Figure 1).
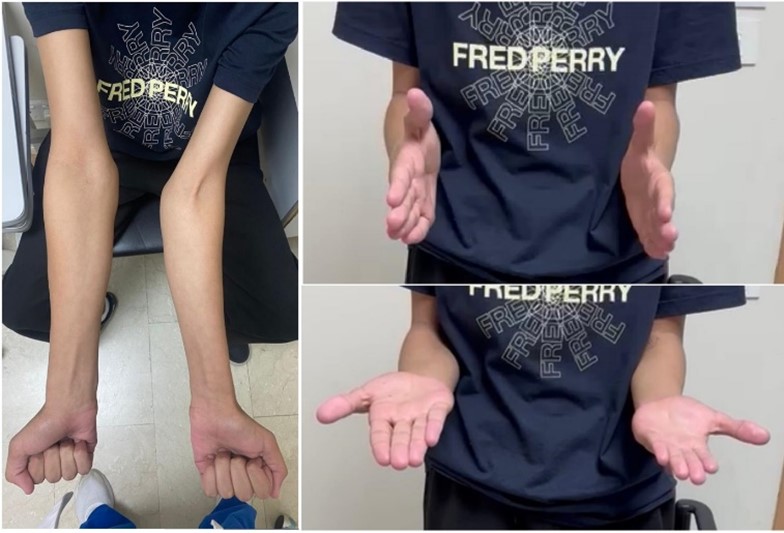
Figure 1: Physical examination during flexion, supination and pronation
The patient was referred for an X-ray, whose findings showed fracture of shaft of ulna, elbow joint deformation and radial head dislocation (Figure 2). The patient was then further referred for a CT scan, which revealed radial head dislocation and radiocapitillar joint degenerative change, confirming the diagnosis of a missed Monteggia fracture (Figure 3).
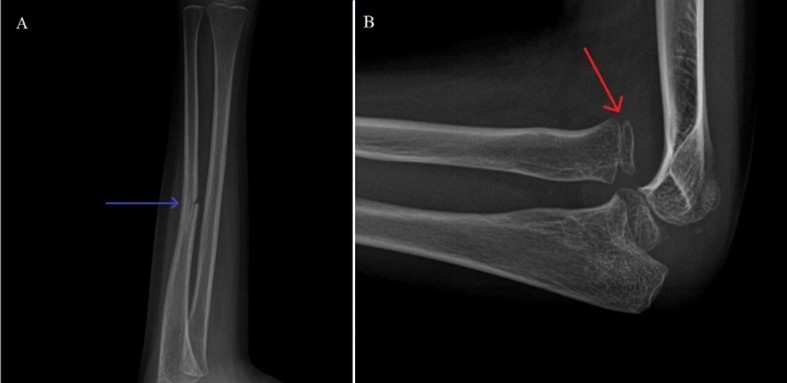
Figure 2: X-ray forearm AP view (A) and lateral view (B) shows fracture of shaft of ulna (blue arrow) and dislocation of radial head and misalignment of radial head with the capitellum (Red Arrow).
Figure 3: Computed tomography of forearm coronal view (A) and 3D (B) shows antero- lateral dislocation of the radial head along with head and misalignment of radial head with the capitellum.
In addition, a magnetic resonance imaging was done to explore the extensive musculoskeletal injury and showed no soft tissue injury (Figure 4). The risk and benefits of the surgical treatment were explained to the father, but he was not willing to proceed with surgery and preferred non-operative interventions such as physiotherapy. Recently, the patient has been following up with physiotherapy sessions.
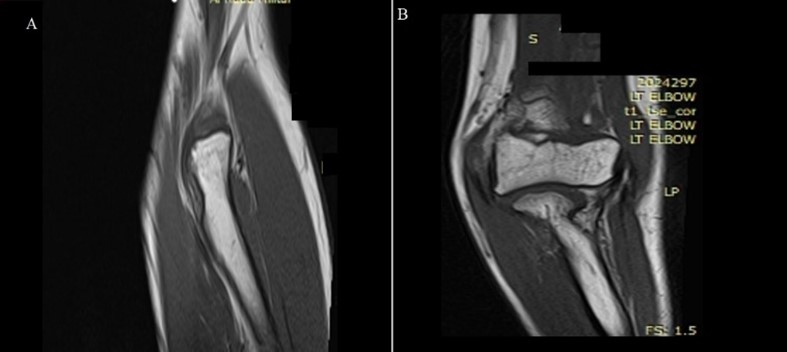
Figure 4: Magnetic resonance imaging of the forearm coronal view (A) and saggital view (B) shows dislocation of the radial head without any soft tissue damage.
Discussion
The precise injury documented and published by Giovanni Battista Monteggia in 1814, consisting of a proximal ulna fracture and radial head dislocation, was, in fact, a description of a neglected injury. The majority of Monteggia fractures in children can be treated conservatively with closed reduction and cast immobilization if adequately detected at the time of injury. Failure to recognize the fracture or injury is the most serious complication. Radial head dislocation is frequently overlooked, and the injury is misdiagnosed as a simple ulnar fracture, an incredibly rare lesion in childhood. Furthermore, plastic deformation of the ulna may go unnoticed, and the injury may be misdiagnosed as an isolated radial head dislocation, another relatively rare disorder in children. Surgery may be required in cases of irreducible radial head dislocation or unstable ulna fracture (6). Similarly, Zhang et al. described that since expectant therapy of neglected Monteggia fractures frequently results in poor outcomes, early surgical intervention is strongly advised to reduce complications. The surgical treatment attempts to cure the ulnar angular deformity, stabilize the radial head, and restore appropriate radiocapitellar joint alignment. Despite the fact that multiple studies have reported diverse treatments for neglected Monteggia fractures, which vary from position to conduct osteotomy, fixation alternatives, and annular ligament restoration, there is still no standard procedure or guidelines (7).
Additionally, Ladermann et al. narrated that due to the lack of joint constraint in cases of missing Monteggia fractures, the radio-capitellar articulation will progressively suffer dysplastic alterations, resulting in well-documented long-term implications that are unsatisfactory for the patient. As a result, the radial head must be reduced (8). Moreover, the findings of a systematic review concluded that unless there is radial head dysmorphism, open reduction should be attempted. The most common technique is open reduction with ulnar osteotomy with or without annular ligament restoration, which is predicted to result in less pain and elbow deformity (9). Furthermore, Aslan et al. described that neglected Monteggia fractures have been deemed irreducible after 2 years of injury due to morphological changes in the capitellum and radial head. A neglected Monteggia fracture will impair not only the elbow but also the distal radioulnar joint and the wrist in the long run. As a result, treating this abnormality is critical for avoiding complications in the future (10). In our case, the Monteggia fracture remained unrecognized/undiagnosed for five years. Surgical management was offered to the patient, but the parents refused and hence opted for the physiotherapy sessions as an alternate management therapy. In the literature, most cases reported of neglected Monteggia fractures were successfully treated with surgical intervention and rarely with physiotherapy alone. Dandi et al. stated that chronic Monteggia fractures result in limited range of motion due to elbow pain, neurologic impairments, and valgus deformity (11). However, in our patient, no neurological or other significant complications were noted except for a limited range of motion.
Alajmi et al. presented three cases of neglected Monteggia fractures in patients aged 5, 4, and 9 years. The patients presented at 10, 20, and 25 days after their injuries. Each of the cases was handled individually, with the final case necessitating open reduction and annular ligament restoration. Following up on all three cases had excellent outcomes (12). Cevi K et al. reported 18 cases of missed fractures, and the average time between injury and surgical management was 8.3 weeks. All surgical procedures went well without any major complications. All patients reported painless forearm and elbow range of motion, as well as a diminished radiocapitellar joint. The authors further recommended that because conservative therapy for this injury may result in significant morbidity, surgical care should be prioritized. The ulnar deformity is a critical site for radiocapitellar joint reduction. The preferred treatment technique has minimal impact on the results as long as it reduces the radial head (13). Contrary to the management of these cases, we managed the case with physiotherapy sessions alone; however, the period of neglected Monteggia fracture in our patient seems to be quite long in comparison to the cases reported in the literature.
Soni et al. narrated that despite the rarity of Monteggia fractures, their greatest significance stems from the fact that the diagnosis is frequently erroneous, with up to 50% of cases being overlooked, particularly in situations with radial head dislocation coupled with a plastic deformation or a greenstick fracture of the ulna. Another factor that contributes to the increased number of chronic Monteggia cases is the loss of the initial reduction, which may account for almost 20% of cases. Neglected Monteggia fracture-dislocation may progress with pain and movement limitations due to an incorrect diagnosis of the initial trauma (14). He et al. commented that delayed diagnosis and treatment of radial head dislocation will result in the traditional challenges of Monteggia fracture treatment. If the displaced radial head is not addressed, it causes elbow pain, limited elbow motion, a growing valgus deformity, and neurologic issues. To correct Monteggia injuries, an ulna osteotomy will be required, causing significant stress to those patients. However, early diagnosis and treatment of Monteggia fractures result in excellent outcomes and allow for conservative therapy in most patients, without the need for complex surgical procedures such as ulna osteotomies or annular ligament repair or reconstruction. When the diagnosis is delayed, however, several pathologic alterations may occur to inhibit radial head reduction (15).
The X-ray and CT scan findings in our case revealed radial head dislocation and radiocapitillar joint degenerative change, which confirmed the diagnosis of a neglected Monteggia fracture that had been missed five years ago when our patient suffered an ulnar shaft fracture. However, due to the refusal of parents, the patient could only be managed through physiotherapy sessions, which makes our case quite unique to present since it is the only case reported to the best of our knowledge with the longest time duration of neglected Monteggia fracture and was managed with physiotherapy sessions alone. However, the management strategy adopted by us could not be compared to other cases since almost all were managed through surgical interventions.
Conclusion
The Monteggia fracture in our patient remained neglected for five long years and caused limited range of motion; however, no other significant or neurological complications were noted. Alternative management strategies, including rehabilitation for Monteggia fractures, need to be studied further to generate evidence-based findings and outcomes. Additionally, their safety and efficacy also need to be determined so more innovative management options are available and offered to patients to achieve optimal outcomes.
Disclosure
Conflict of interest
There is no conflict of interest.
Funding
No funding
Ethical consideration
An informed written consent was taken from the patient to report this case without revealing any personal information and an ethical approval was obtained from Al Hada Military Hospital in Taif to publish this case.
Data availability
Data that support the findings of this study are embedded within the manuscript.
Author contribution
All authors contributed to clinical assessment, data collection and final drafting and proofreading of the case.