Volume 1, Issue 4
July 2021
Osteoporosis Awareness in Saudi Arabia: A Systematic Review of Cross-Sectional Studies
Marwah Abdullah, Ali Haddadi, Faten Madkhali, Turki Sahhari, Ali Al Obaid, Fahad Aljabry, Adel Albeladi, Suzan Mulla, Samah Al Swaidan, Jumana Al kaf, Abdulmohsen Shaikh
DOI: http://dx.doi.org/10.52533/JOHS.2021.1403
Keywords: cross-sectional, osteoporosis, knowledge, awareness, attitude, saudi arabia
Saudi investigations reported that the application of preventive approaches to limit the spread of osteoporosis is poor. This indicates the importance of nationwide investigations to stress the importance of the adequate implementation of preventive measures. A thorough electronic search of a wide range of databases was conducted to identify all the relevant cross-sectional studies reporting knoweldge, awareness and practice among Saudi population, with no time limitations. A total of 25 prospective cross-sectional studies that were conducted in Saudi Arabia were included and were published between 2010 and 2021. Most of these studies were conducted in Riyadh, however, other regions such as Bisha, Qassim, Taif, Al-Hassa, Alahsa, Jazan, and nationwide can also be found in our included studies. The sample size was hugely variable and ranged between 43 and 1,830, with a total of 12,407 individuals. Among the included studies, 11 included female populations only, 3 included healthcare workers only, and the rest included mixed populations. Most of the included studies had good awareness levels regarding osteoporosis. Moreover, we also found that age, gender, education level, and socio-economic status are common factors that may impact the level of knowledge and awareness across the different studies, although some studies reported the non-significance of these variables. Further education campaigns are still needed to further enhance levels of awareness of other factors than the ones reported.
Introduction
The term “silent disease” has been used to describe osteoporosis as many osteoporotic patients have an asymptomatic progression of the disease and are not usually aware of the impact of the disease on their bones until complications such as fractures occur (1). Deteriorated bony structures, lost bone mineral density, bone fagility, and fracture potential are the main hallmarks of osteoporosis alongside the course of the disease (2). As a result of the potential complications and fractures, significant morbidities, mortalities, and cost burdens for the affected patients and the corresponding healthcare systems have been reported in the literature (3). Annually, around nine million global cases of osteoporosis-induced fractures have been estimated (4).
Worldwide estimates indicate that around 200 million female patients have been diagnosed with osteoporosis (5). Reports also show that one and two in every five Caucasian males and females will eventually suffer from osteoporosis-induced fractures during their life, respectively (3). In Saudi Arabia, estimates show that the prevalence of osteoporosis is high, at 30.7% and 34% in males and females, respectively, and the rate is expected to increase in the coming years (6). Aging, smoking, increased consumption of caffeine, immobilization, having a family history of osteoporosis-induced fractures, reduced intake of adequate amounts of calcium and vitamin D, sedentary lifestyles, and being Asian or White, among many other factors, have been associated with the development of osteoporosis (3). Previous studies have demonstrated that being aware and acquiring adequate knowledge about the risk of osteoporosis as well as enhancing lifestyle choices can lead to significantly enhanced prevention against the disease (7-10).
Many global studies have been published to assess the levels of knowledge and awareness of osteoporosis among different populations. For instance, a previous study from Egypt reported that only a third of their elderly female population were aware that osteoporosis could be adequately managed (11). Another study from Australia showed that having a family history of osteoporosis and living in rural areas was associated with lower knowledge scores regarding osteoporosis (12). Previous studies have also been conducted in Saudi Arabia to assess the level of awareness. For instance, a study showed that only 58% and 44% of the included male and female Saudi population, respectively, were aware that osteoporosis is a silent disorder (13). Other investigations reported that the utilization of effective preventive methods in limiting the spread of osteoporosis is scarce (14, 15). This indicates the importance of nationwide investigations to stress the importance of adequate implementation of preventive measures. Therefore, we aimed to collect nationwide evidence about the awareness of the different Saudi populations towards osteoporosis, based on the evidence from previously published cross-sectional investigations.
Methods
Inclusion and exclusion criteria
We aimed to assess the knowledge and awareness of the Saudi population towards osteoporosis according to previously published cross-sectional investigations across the Kingdom. We included studies that were original cross-sectional studies, investigated human subjects, conducted in Saudi Arabia and investigated the knowledge or awareness of osteoporosis within the Kingdom of Saudi Arabia. On the other hand, we excluded citations during our screening if they were non-original or non-cross-sectional investigations, non-human-based studies, not conducted in Saudi Arabia, and did not adequately investigate the level of knowledge or awareness about osteoporosis among the included population.
Search strategy
The search and conduction of this study was based on the previous recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (16). The following search term: (Knowledge OR attitude OR practice OR aware*) AND osteoporosis AND ("Saudi Arabia" OR Saudi) was used based on the keywords that were retrieved from previous relevant investigations to find all the relevant studies in PubMed. We also searched other databases using these keywords, however, the search strategy was continuously adjusted based on the terms and conditions that were provided by each database to obtain proper results. Among the available databases, we searched Virtual Health Library, Embase, Google Scholar, Cochrane Library, Web of Science, and Scopus. Finally, we also performed a manual search within the references of the included studies and relevant reviews to adequately expand our search strategy so as not to miss any relevant articles that could be relevant to our intended aim (17, 18).
Screening and data extraction
A vital step in this study was to identify the relevant articles which we would then use to extract the relevant information that could help us formulate our evidence about our intended aims and outcomes. Accordingly, after all the results of the search strategy were imported into a single file, and after all the duplicates were removed, we designed a sheet that was by the study authors to screen the imported citations, first by titles and abstracts, and then by full-texts. Each of these steps was undertaken by at least four members who drew on group discussions to reach a final decision whenever a conflict arose. After deciding to include the final list of the relevant articles, the next step was then planned by piloting an extraction sheet that was used for all the included studies to retrieve all the relevant information. The sheet was formed of three parts: 1) characteristics and study settings by exctracting the first author’s last name, the title of the article, and its given identification to properly identify it, study design, sample size, setting of the study, nature of data collection, age and gender, 2) the relevant outcomes, including the knowledge and awareness of osteoporosis, the attitude of the population towards the disease, and the associated factors, and 3) the quality assessment, which will be discussed in the following paragraph.
Quality assessment
To perform this step, all the domains of the modified Newcastle-Ottawa scale (mNOS) for cross-sectional studies (19) were imported into an excel sheet in accordance with a proper explanation for each to facilitate the task for all members and to make this an easy and accurate step. Assessment of outcomes, methods, compatibility, and selection of participants were the main domains of the tool, by which studies were graded by their total scores into satisfactory or not, and good or excellent in quality, indicating the lowest to the highest degree of bias. The results of the risk of bias are interpreted in the following sections.
Results
Search results
In Figure 1, we have summarized the results of the search and screening strategies based on the PRISMA guidelines. In brief, we found a total of 451 relevant citations from all of the relevant databases where we applied our search strategy. After screening, a total of 20 articles were found to be relevant to our aim and outcomes, and the final list consisted of 25 articles as we identified an additional five using the manual search of the relevant studies and reviews.
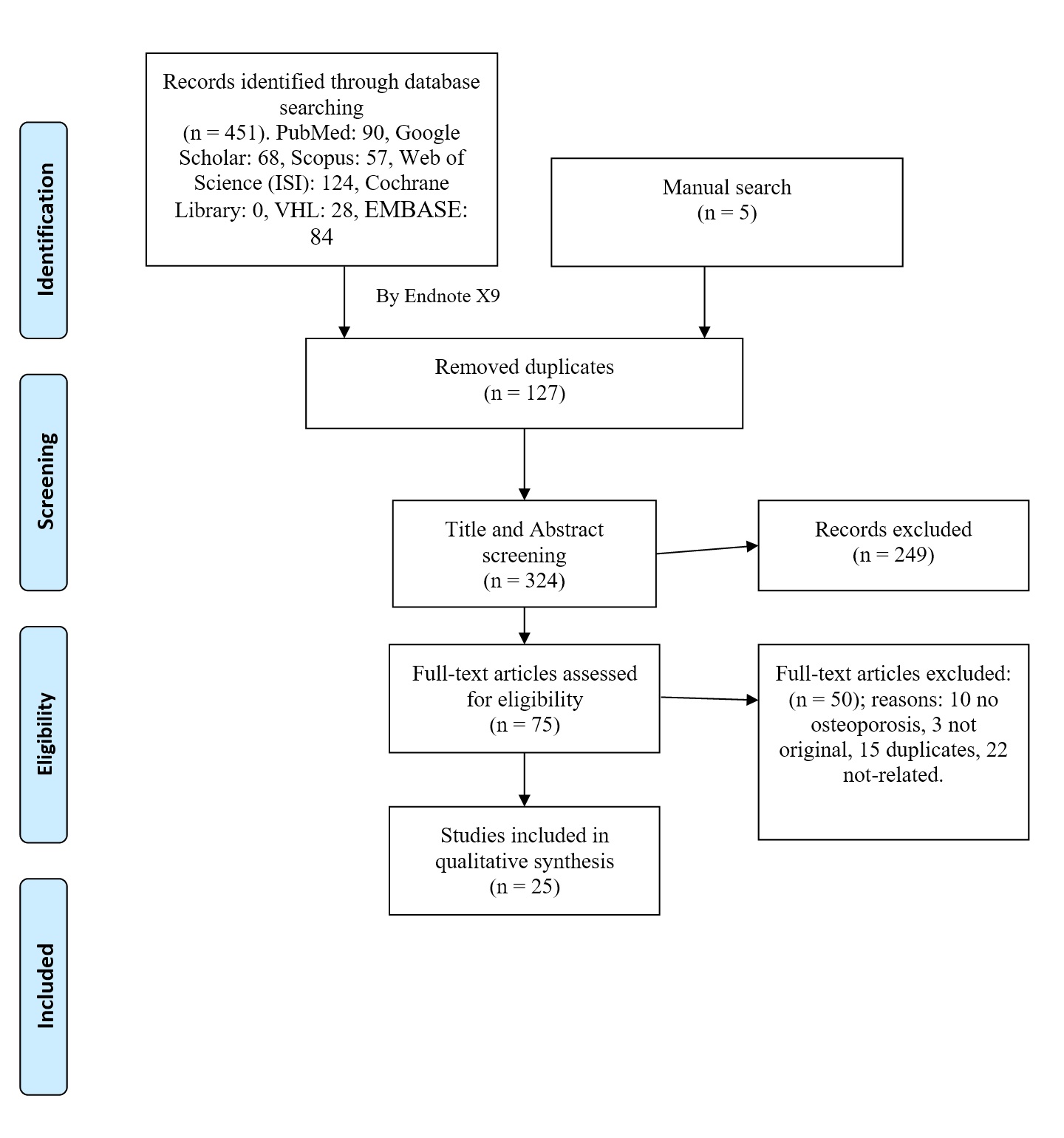
Figure 1. PRISMA flow diagram for study selection and search strategy.
Results of quality assessment
According to the results of the assessed quality based on the modified NOS tool, only four studies had a non-satisfactory rating, indicating the significant risk of bias among these studies. Seven studies had a good rating, indicating the low risk of bias in these studies, while the rest of the included studies were assessed as having a satisfactory rating. The detailed results of the risk of bias assessment are presented in Table 1.
Table 1. Quality assessment and domains of the modified Newcastle-Ottawa scale (mNOS) for cross-sectional studies.
|
Author |
Year |
Selection |
Comparability |
Outcome |
Total score |
Quality |
||||
|
Representativeness of the Sample |
Sample size |
Non-Respondents |
Ascertainment of the Exposure |
The Subjects in Different Outcome Groups are Comparable |
Assessment of outcome |
Statistical analysis |
||||
|
Ahmed et al.(20) |
2020 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Aladwani et al.(21) |
2019 |
+ |
+ |
+ |
+ |
4 |
Non-satisfactory |
|||
|
Alamri et al.(22) |
2015 |
+ |
+ |
+ |
+ |
++ |
+ |
+ |
8 |
Good |
|
Alghamdi et al.(23) |
2018 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
|
Al-Ghamdi et al.(24) |
2017 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
|
Alghunaim et al.(25) |
2016 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Alharthi A.(26) |
2018 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
AlHarthi B.(27) |
2017 |
+ |
+ |
+ |
+ |
4 |
Non-satisfactory |
|||
|
Almutairi (28) |
2021 |
+ |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
|
|
Al-Otaibi (29) |
2015 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
|
Alqahtani and Alghamdi(30) |
2021 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
|
Alsaleem et al.(31) |
2020 |
+ |
+ |
+ |
+ |
4 |
Non-satisfactory |
|||
|
Alshahrani et al. (32) |
2020 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
|
Al-Shahrani et al.(33) |
2010 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
|
Alshammari (15) |
2014 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
|
Alshareef et al.(34) |
2018 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
|
Barzanji et al.(35) |
2013 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
|
Darout et al.(36) |
2017 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Khalifa et al.(37) |
2016 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
|
Khan et al.(38) |
2019 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Khired et al.(39) |
2021 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
|
Saeedi et al.(40) |
2014 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Utkarsh et al.(41) |
2018 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Tlt et al.(13) |
2016 |
+ |
+ |
+ |
+ |
4 |
Non-satisfactory |
|||
|
Tripathi et al.(42) |
2018 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
Studies’ main characteristics
All of the 25 included studies were prospective cross-sectional and were conducted in Saudi Arabia. All studies were published between 2010 and 2021. Most of these studies were conducted in Riyad, however, other regions as Bisha, Qassim, Taif, Al-Hassa, Alahsa, Jazan, and nationwide were also found in our included studies. The sample size was hugely variable and ranged between 43 and 1,830, with a total of 12,407 individuals. Among the included studies, 11 included female populations only, 3 included healthcare workers only, while the rest included mixed populations. The authors’ conclusions and detailed characteristics of these studies are presented in Table 2.
Table 2. Baseline characteristics and authors’ conclusions for the included investigations.
|
Reference |
Year |
Region |
Sample size |
Male (n) |
Mean age |
Targeted populations |
Conclusion |
|
Ahmed et al. (20) |
2020 |
Al Majmaah |
43 |
76.70% |
41.5 (4.8) |
General practitioners |
72% believed that osteoporosis has a major impact on health. 77% knew that bisphosphates are the most commonly prescribed drugs. |
|
Aladwani et al.(21) |
2019 |
Riyadh |
385 |
58.20% |
- |
General population |
Low knowledge scores. Significant factors included. educational level but not age or gender. |
|
Alamri et al.(22) |
2015 |
Nationwide |
1830 |
58% |
36.7 (13.6) |
General population |
78% heard about osteoporosis. Increased practice of preventive measures was associated with the awareness levels. Age, gender, education, residence, income, and occupation were significant factors. |
|
Alghamdi et al.(23) |
2018 |
Bisha |
141 |
63 |
38.17 (9.6) |
Healthcare workers |
Around 90% had good knowledge about osteoporosis. No reported factors. |
|
Al-Ghamdi et al.(24) |
2017 |
Riyadh |
500 |
0 |
26.58 (10.19) |
Female general population |
82% had excellent levels of knowledge about osteoporosis. Significant factors are college status, having heard about osteoporosis, and marital status, but not age, social level, or educational level. |
|
Alghunaim et al.(25) |
2016 |
Qassim |
986 |
46% |
28.6 (9.1) |
General population |
Females had better knowledge than males. |
|
Alharthi A. (26) |
2018 |
Taif |
986 |
46% |
28.6 (9.1) |
General population |
Most participants had good knowledge about osteoporosis. Age was inversely proportional to knowledge, educational status. |
|
AlHarthi B.(27) |
2017 |
Riyadh |
200 |
0 |
21->41 |
Female general population |
Most participants had good knowledge about osteoporosis. Age, economic status, and educational level |
|
Almutairi (28) |
2021 |
Al Majmaah |
316 |
66.80% |
18-60 |
General population |
Moderate knowledge about osteoporosis. Educational level, marital status, nationality, gender, and employment were significant factors. |
|
Al-Otaibi (29) |
2015 |
Al-Hassa |
288 |
0 |
20-40 |
Female general population |
Moderate knowledge about osteoporosis. Reduced calcium intake and exercise. Family history was the sole factor. |
|
Alqahtani and Alghamdi (30) |
2021 |
Riyadh |
376 |
0 |
18->45 |
Female general population |
Most participants had good knowledge about osteoporosis. Old age is associated with higher scores |
|
Alsaleem et al.(31) |
2020 |
Eastern region |
1100 |
0 |
- |
Female general population |
Most participants (60.3%) had poor knowledge scores. Age, educational level, and residency were significant factors. |
|
Alshahrani et al. (32) |
2020 |
Riyadh |
69 |
18.8 |
32 (8.66) |
General population and caregivers |
The mean score was 16.28 out of 33 which was unsatisfactory. Higher educational levels and being a caregiver were significant factors. |
|
Al-Shahrani et al.(33) |
2010 |
Riyadh |
368 |
0 |
NS |
Female general population |
62% knew about osteoporosis, poor to fair levels of identification of the risk factors was noticed, 48% identified calcium-rich foods. Young age and educational levels were significant factors. |
|
Alshammari (15) |
2014 |
Riyadh |
500 |
0 |
33.59 (6.86) |
Female university students |
Included women had satisfactory knowledge scores. Knowledge is associated with attitude. Marital status, age, employment, drinking coffee, and number of children were significant factors. |
|
Alshareef et al.(34) |
2018 |
Riyadh |
1012 |
0 |
18-30 |
Female university students |
Around 80% had inadequate knowledge. Reduced attitude based on the level of knowledge. Monthly income and accommodation status were significant factors. |
|
Barzanji et al.(35) |
2013 |
Riyadh |
505 |
246 |
33.78 (10.46) |
Adult general population |
The mean knowledge score was 56.6%, which is not adequate and further educational campaigns are needed. Reduced sticking to the preventive measures especially among females. Employment, educational level, and income were significant factors. |
|
Darout et al.(36) |
2017 |
Jazan |
546 |
0 |
<20-50 |
Female healthcare and healthcare participants |
54.3% of non-healthcare and 61.9% of healthcare workers had good scores, respondents had adequate knowledge about preventive measures but reduced knowledge about attitude sunlight exposure, and vitamin administration. Age was the sole factor. |
|
Khalifa et al.(37) |
2016 |
Riyadh |
150 |
67.30% |
- |
General population |
Most participants heard about osteoporosis, and two-thirds had moderate knowledge. Around half of the population knew they were susceptible to osteoporosis. Gender and the level of knowledge were significant factors. |
|
Khan et al.(38) |
2019 |
Jeddah, Tabuk, Taibah, Mekkah |
337 |
161 |
18-30 |
University students |
92% had some level of awareness and around 50% had good levels. Educational level and gender were significant factors. |
|
Khired et al.(39) |
2021 |
Riyadh |
250 |
0 |
17-25 |
Female university students |
16% only had adequate knowledge. A small proportion engaged in the preventive measures. Media had a negative correlation with knowledge. |
|
Saeedi et al.(40) |
2014 |
Riyadh |
364 |
70% |
39.5 (9.1) |
Healthcare workers |
Most participants were aware of osteoporosis. Most participants did not know about preventive guidelines of osteoporosis, but a big proportion knew about the standardized screening tool. |
|
Utkarsh et al.(41) |
2018 |
Al-Ahsa |
176 |
0 |
21.46 (1.54) |
Female University medical students |
65.1% had satisfactory knowledge scores and less than one-third had poor scores. Age, educational level and marital status were significant factors. |
|
Tlt et al.(13) |
2016 |
Nationwide |
579 |
27.12% |
15->65 |
General population |
Low knowledge scores. Negative attitudes towards screening and prevention of risk factors. |
|
Tripathi et al.(42) |
2018 |
Jazan |
400 |
29.50% |
NS |
General population |
The majority of the participants were aware of the risk factors, causes, and symptoms of osteoporosis. The practice of prevention was poor but dietary intake was favorable and the majority knew that they were susceptible to osteoporosis. Age and the level of education were significant factors. |
Discussion
In Riyadh, a previous investigation by Alqahtani and Alghamdi (30) reported that the overall knowledge of osteoporosis in their adult female population was good in approximately two-thirds of the population. The authors also reported that being younger (<40 years old) was associated with reduced knowledge and awareness of osteoporosis in their population. Another study by Khired et al. (39) also reported that only 16% of the included female students had good knowledge scores, and only 49% were aware that osteoporosis could induce significant adverse outcomes. The main item where knowledge was hugely low was the risk factors that are associated with the disease. In addition, the authors reported that only a few of the participants were engaged in routine physical activities and consumption of daily products. Barzanji et al. (35) also reported that most of the study participants (86%) had heard of osteoporosis, and the mean knowledge score was 56.6%. Residency, employment, and education levels were associated with the level of awareness of osteoporosis. The authors reported that the knowledge of osteoporosis among their male and female population was inadequate among a considerable number, which required the integration of adequate preventive measures. Alshahrani et al. (32) also reported that the level of knowledge and awareness among their population was not satisfactory and the estimated mean knowledge score was 16.28 out of 33. The authors also reported that being a caregiver and highly educated were both significant factors that were associated with higher knowledge scores. In a previous investigation by Alshammari (15) both working and housewife women had good knowledge scores of osteoporosis, however, their attitudes were non-satisfactory. The level of knowledge was significantly correlated to a positive attitude towards the preventive measures. In another study by Al-Shahrani et al. (33), 62% of the study participants were aware of osteoporosis, and only 48% identified foods that are rich in calcium. Younger ages were associated with higher knowledge scores and poor to fair judgments were given for the study participants for their abilities to identify the risk factors of the disease. Al-Ghamdi et al. (24) reported that 82% of their female population had excellent levels of knowledge of osteoporosis. College status, marital status, and having previously heard of osteoporosis were significantly different among the study population. On the other hand, neither age, social status, nor education level were significant factors that could be associated with the level of knowledge, which is unlike the other previous investigations. Alshareef et al. (34) also indicated that most of the female university students in the study population did not have adequate knowledge of osteoporosis. Khalifa et al. (37) reported that almost all of the study population (145/150) had heard of osteoporosis and only 25% of the study population had good knowledge scores, while more than 60% had moderate knowledge scores. The authors also indicated that the levels of knowledge among the male group were higher than the female group in assessing their knowledge in the most likely susceptible age group to develop osteoporosis. However, there was no significant difference between the two groups in terms of thinking that they could develop osteoporosis later on in their life. Moreover, the level of knowledge of osteoporosis was associated with the attitude towards ingestion of foods that can prevent the development of osteoporosis. In 2017, AlHarthi B (27) reported that the prevalence of good knowledge scores among the study population was high, and age, socioeconomic level and level of education were all significantly associated with the levels of knowledge among the study participants. Among primary healthcare physicians, Saeedi et al. (40) reported that 81% of their population reported that osteoporosis is a significant clinical problem, while 84% were not aware of the presence of clinical guidelines to manage osteoporosis. Most of the study participants were aware of the screening methods for osteoporosis and of their potential roles for preventing the disease. Aladwani et al. (21) reported that neither age or gender were associated with the level of knowledge of osteoporosis, but education level was.
In Al-Hassa, Al-Otaibi (29) reported that the estimated mean knowledge scores in their female population were moderate, and having a family history of osteoporosis was significantly associated with higher knowledge scores. The authors also reported that calcium intake was inadequate among the study population and increased intake was associated with a family history of osteoporosis. A nationwide investigation among university students by Khan et al. (38) also reported that around 92% of their students had some knowledge of osteoporosis, and approximately 50% had good to high knowledge scores. Moreover, they reported that high knowledge scores correlated with being female and having a higher education level. Another nationwide investigation by Almari et al. (22) also reported that 78% of their population had heard of osteoporosis. Additionally, the authors also reported that the assessed socio-economic factors in their population were significantly associated with the scores of these participants. Tlt et al. (13) also conducted a similar investigation to find that 58% to 44.4% of the male and female participants, respectively, knew that osteoporosis is a silent disease. Moreover, reduced ingestion of calcium-rich foods was the most commonly identified risk factor for osteoporosis while previous hip fractures were the least commonly identified factor. More than two-thirds of the study participants believed that they would have osteoporosis later on in their lifetime. Among healthcare workers, a study by Alghamdi et al. (23) showed that most healthcare workers in their investigation were assessed to have high and adequate knowledge scores of osteoporosis. Among female medical students in the Al-Ahsa region, Utkarsh et al. (41) reported that only 2.3% of the study population had good knowledge scores, and 32.2% and 65.15 had poor and satisfactory levels of knowledge of osteoporosis, respectively, and therefore, the level of knowledge was considered low in this study when compared to international investigations.
In Jazan, Darout et al. (36) reported that approximately 54% of non-healthcare workers and 62% of healthcare workers had adequate and good knowledge and awareness levels of osteoporosis, respectively. The authors also reported that more than half of their population were aware of the preventive dietary regimens, while approximately 48% and 44% of the healthcare and non-healthcare workers had inadequate knowledge of behavior and attitude of osteoporosis, respectively. Tripathi et al. (42) also indicated that most of the study participants were aware of the symptoms, causes, and risks of osteoporosis. Higher knowledge scores and positive attitudes were associated with females, individuals that were <30 years of age, and higher education levels. In the Taif region, Alharthi reported that most of the study participants had high knowledge levels of osteoporosis, however, the level of knowledge was inadequate in some areas. Moreover, the study reported that female participants and younger individuals had higher scores than the rest of the population (26). In the Qassim region, Alghunaim et al. (25) reported that most of their female population had adequate knowledge of some aspects of osteoporosis, and age, gender, and education level were significantly associated with the level of knowledge among the study participants. In Al Majmaah province, Ahmed et al. (20) reported that most of the study population of general practitioners had good knowledge scores regarding osteoporosis and they believed in the beneficial role of the application of adequate preventive measures. Moreover, 72.1% of the study population were aware that osteoporosis has a significant impact on the health of the affected patients. Another investigation in Al Majmaah region by Almutairi (28) reported that the level of knowledge among the study participants was moderate and approximately 39% had good knowledge scores, while around 61% had poor scores, and 77% had previously heard of osteoporosis. In the eastern region, Alsaleem et al. (31) reported that age, residency, and education levels were not significantly associated with the level of awareness, unlike socioeconomic levels. The authors also reported that despite the high levels of knowledge among their study population of females, only 2.3% had good knowledge scores, while 37.5% and 60.3% had moderate and poor knowledge scores, respectively.
Our study is limited by the small sample size of some included investigations and the reduced representativeness of these studies of the different regions across the Kingdom, as most studies were conducted in Riyadh. Moreover, the low quality of some studies is a further limitation, indicating the need to inaugurate further nationwide studies with proper sampling and a lower risk of bias.
Conclusion
Although some studies have reported that most of their population had good awareness levels of osteoporosis, further education campaigns are still needed to further enhance the levels of awareness and achieve better interventions. Moreover, we also found that age, gender, educational level, and socio-economic status are common factors that may impact the level of knowledge and awareness across the different studies despite some studies that reported the non-significance of these variables, which further indicates the need for larger investigations.
Declaration
Statement:
The authors declare no conflict of interest.
Funding:
None.
Ethical Consideration:
None applicable.
Data Availability:
All data is available withing the article.
