Volume 1, Issue 4
July 2021
Down Syndrome Children Feeding Habits in Saudi Arabia: A Systematic Review
Abdulaziz Alradha, Naqa Sulis, Joud AlYousha, Mohammad Alzaher, Ahmed Alzaher, Abdulaziz Almutairi, Zahra Alshuwaikhat, Abrar Aldawood, Raghad Alturaifi, Khalid Alqahtani, Mohammed Alisi
DOI: http://dx.doi.org/10.52533/JOHS.2021.1405
Keywords: down syndrome, trisomy 21, nutrition, breastfeeding, saudi arabia, systematic review
It is widely accepted that establishing healthy feeding habits for children is the best prevention against future disease, and as a result of the potential comorbidities with Down syndrome, these patients are more likely to develop abnormal lifestyle habits. Few studies have assessed the feeding habits among Saudi children with Down syndrome. Therefore, we aimed to conduct the current systematic review to collect all the potential evidence regarding the feeding habits of children with Down syndrome in Saudi Arabia. We conducted a systematic search to find relevant articles through EMBASE, PubMed, Google Scholar, Cochrane Library, Scopus, Virtual Health Library, and Web of Science databases. The relevant outcomes were then extracted from the included articles and discussed within the manuscript. We found four relevant articles that met our inclusion criteria, all of which were prospective cross-sectional and were conducted in Riyadh. The studies were published between 2006 and 2013, with a total sample of 892. Our results indicate that the rate of exclusive breastfeeding is relatively high among our population and it also lasts for an acceptable duration during infancy when compared to worldwide investigations. No solid conclusions can be formulated as a result of the small number of included studies and the heterogeneity in outcomes among them, and therefore, further investigations are encouraged to strengthen the current evidence.
Introduction
Down syndrome is characterized by major mild-to-moderate intellectual and cognitive disabilities that result from an abnormal trisomy involving chromosome 21, or part of it. Estimates show that the disorder usually involves one child in every 800-900 newborn children, however, the prevalence rates are variable across countries and different populations as a result of the variety in the relevant risk factors such as parental screening and maternal age (1, 2). Many characteristics have been reported for patients with Down syndrome, including reduced development of psychomotor functions and increased risk of congenital anomalies, in addition to characteristic phenotypes (3, 4). However, it should be noted that the clinical presentation for all patients is not the same, as some patients may have mild disease while others may suffer from significant complications.
It has been estimated that approximately 45% of children with Down syndrome suffer from congenital heart anomalies, primarily including ventricular and atrioventricular septal defects (5). Furthermore, other reports estimate that around 4-6% of these children suffer from gastrointestinal tract anomalies such as Hirschsprung disease, duodenal atresia, and anorectal malformations (6-8). Coeliac disease is also commonly reported in children with Down syndrome, with variable prevalence rates across different populations. However, a meta-analysis showed that the pooled prevalence of the disease is 5.8%, as compared to a rate of 0.5-1% for patients from the general population (9). Children with Down syndrome are also more prone to developing significant comorbidities such as orofacial dysfunction and hypotonia, which might affect the normal feeding habits in these children (10). In addition, thyroid diseases and autoimmune disorders are also common among these children, which can significantly impair energy metabolism and affect their nutritional status (11, 12).
In this context, previous studies have demonstrated that obesity and feeding issues are commonly associated with Down syndrome (13, 14). Parenteral caring for the nutritional status and habits of their children with Down syndrome is important because these might be associated with several characteristics and co-morbidities that could impact the prognosis of these children. Clinicians should carefully assess the nutritional status of these children for successful interpretation of the condition and planning of dietary advice based on the clinical assessment of these patients (15). In general, it is widely accepted that establishing healthy feeding habits for children is the best prevention against future disease, and as a result of the potential comorbidities with Down syndrome, these patients are more likely to develop abnormal lifestyle habits (16). Not many studies have assessed the feeding habits among Saudi children with Down syndrome. This study aims to collect all the potential evidence regarding the feeding habits of children with Down syndrome in Saudi Arabia.
Methods
Inclusion criteria and intended outcomes
The primary endpoint of the present study is to report the feeding habits and nutritional practices among children with Down syndrome in Saudi Arabia, according to studies that were conducted in this region. Accordingly, we have included studies that were: 1) conducted in Saudi Arabia, 2) assessed the feeding habits and nutritional practices, 3) reported these outcomes for children with Down syndrome, 4) published any time and anywhere across the Kingdom, 5) and with no language restrictions. On the other hand, studies were excluded if they were: 1) not published in Saudi Arabia, 2) did not assess the feeding habits, 3) did not include children with Down syndrome, and 4) not original investigations, as reviews, synthesis, protocols, commentaries, editorials, and others.
Search strategy
All of the steps followed were undertaken per the regulations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (17). We formulated the search strategy by searching various electronic databases including EMBASE, PubMed, Google Scholar, Cochrane Library, Scopus, Virtual Health Library, and Web of Science, using the relevant keywords that we obtained from a pilot search and screening strategy across potentially relevant investigations that assessed similar outcomes to ours. For PubMed, we used this search term: (Feed OR feeding OR fed OR breastfeeding OR breastfed OR breastfeed OR Nutrition OR Nutrients OR nutritional) AND ("Down Syndrome" OR "Trisomy 21"), which was then modified based on the requirements and guidelines of each database to identify all the relevant investigations. We also searched the references of the included studies manually for fear of potentially missing any relevant investigation by the electronic search strategy and the screening steps (18, 19).
Screening steps and data extraction
After importing all the results of the searched online platforms to a single endnote sheet to eliminate all the potential duplicates, all of the remaining studies and citations were then unified in a single excel sheet for our members to ensure the screening steps and the process of identification of the included articles was easy. To avoid bias in the screening assessment, at least two reviewers assessed each article, and after blinding their results from each other, the screening process was also divided into two steps including the title and abstract process and the full-text screening process to make sure not a single article was missed. Any disagreements among members were resolved by a public discussion under the adequate supervision of an experienced member. Data extraction was performed by all the authors of the current study, following all the aforementioned conditions to maintain transparency and avoid bias. The extracted data included three main parts including the baseline characteristics of the included studies, the study outcomes including the rate of breast and bottle feeding, duration of this habit, the introduction of solid foods, and other outcomes in addition to a third tab that was specified for the quality assessment tool.
Quality assessment
The modified Newcastle-Ottawa scale (mNOS) for cross-sectional studies (20) was used to complete this element. All studies were given scores from 0 to 10, and accordingly, they were graded into satisfactory, excellent, good, or non-satisfactory according to the degree of bias among them. Similar to the screening and data extraction, this step was also performed accordingly to maintain the transparency of assessing and reporting the outcomes.
Results
Search results
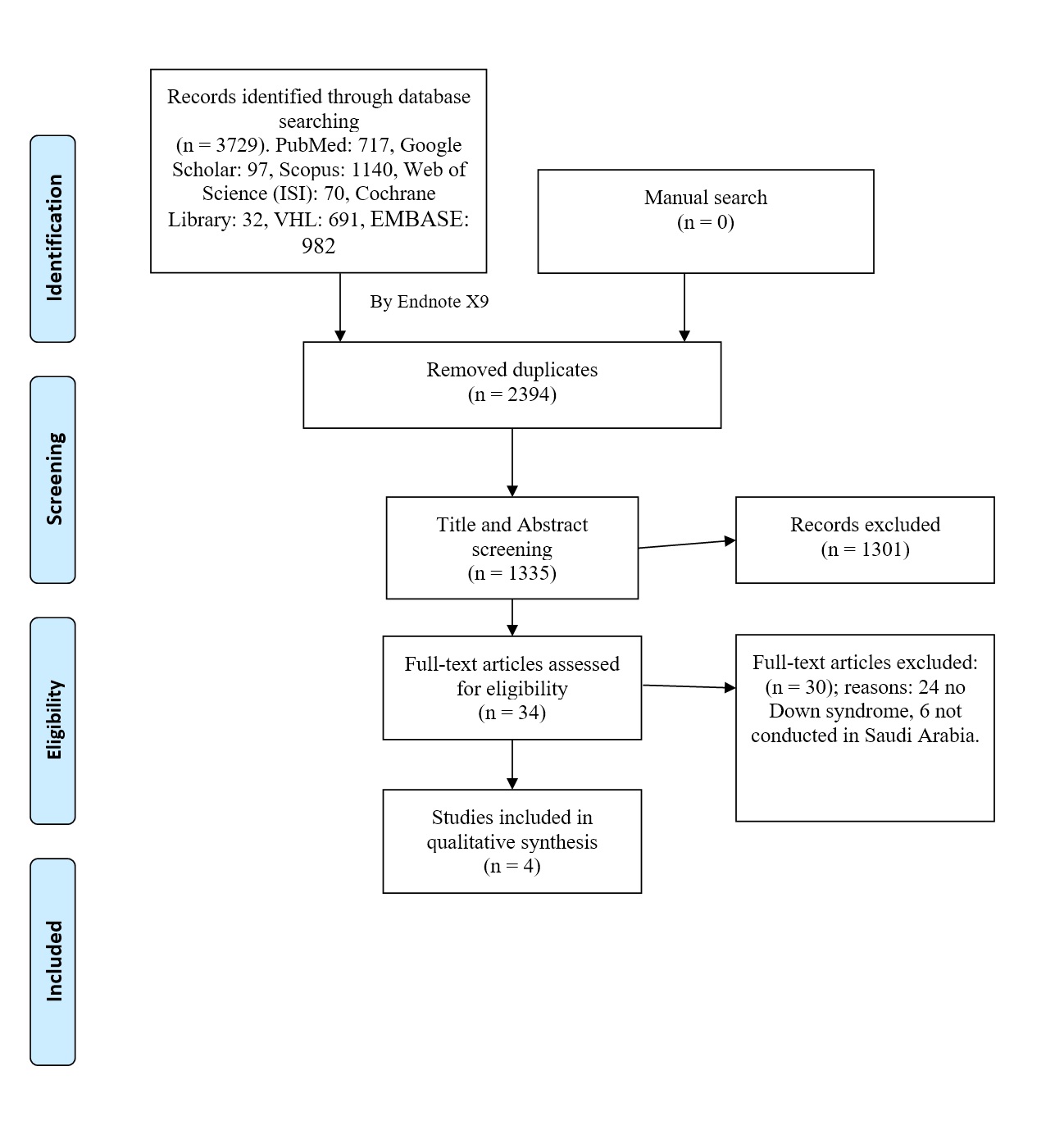
The total number of citations exported from all the databases was 3,729. Among these, 2,394 duplicates were detected and removed using endnote. Following title and abstract screening and full-text screening, we managed to include 4 relevant articles that were in accordance with our inclusion and exclusion criteria. A manual search was also conducted, however, we did not find any missing articles via this method. These steps have been detailed in the PRISMA flow diagram in Figure 1.
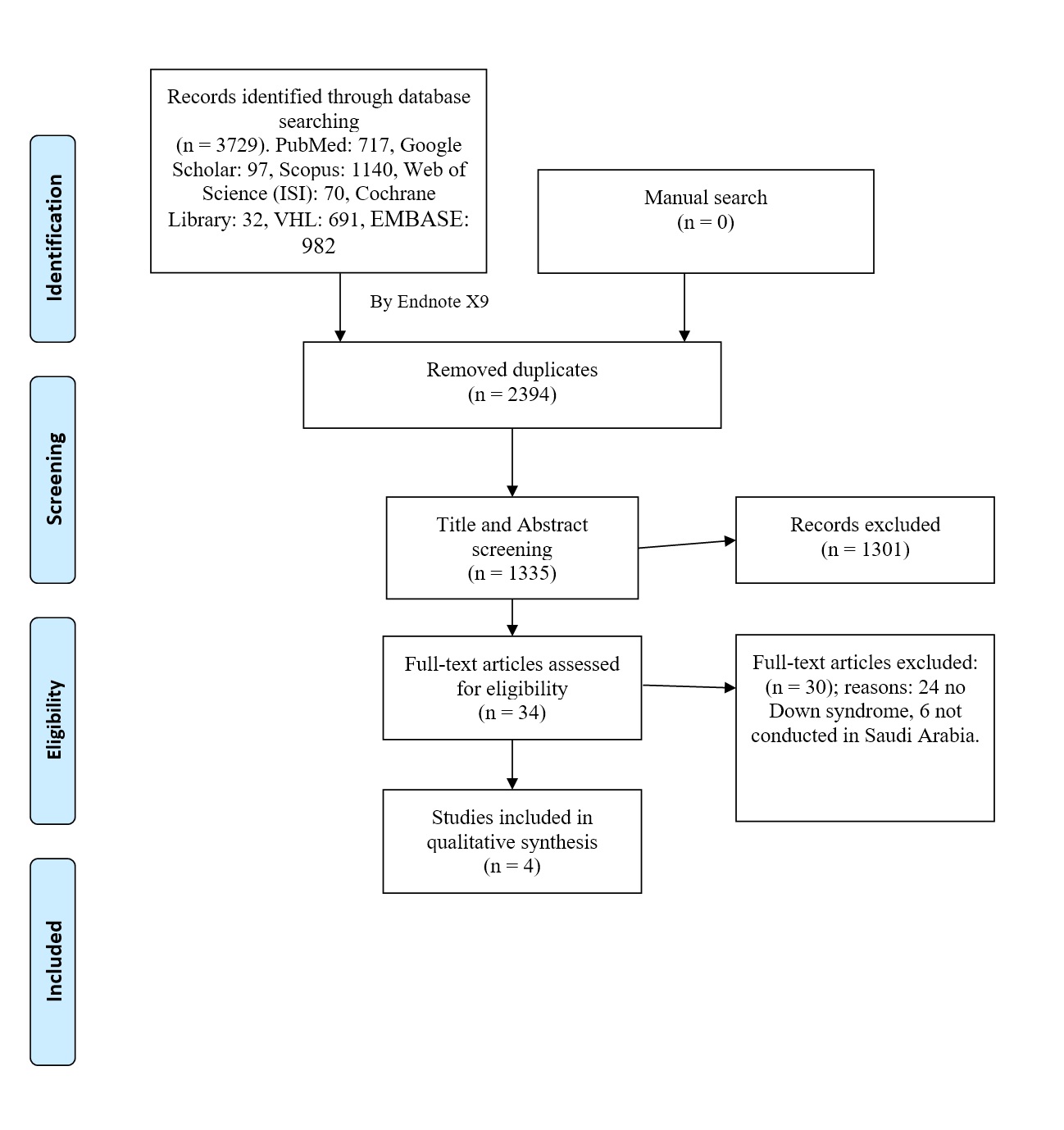
Figure 1. PRISMA flow diagram showing the process of study selection
Characteristics of the included studies
The total number of the included studies was four, all of which were prospective cross-sectional and were conducted in Riyadh through questionnaire-based approaches obtained from the families of the children with Down syndrome. The studies were published between 2006 and 2013, with a total sample size of 892. Detailed baseline characteristics and authors’ conclusions are presented in Table 1.
|
Table 1. Baseline characteristics of the included articles. |
||||||||
|
Reference |
Year |
Setting |
Region |
Sample size |
Age |
Targeted populations |
Authors' conclusions |
|
|
Mean (SD) |
Male/female |
|||||||
|
Al-Sarheed et al. (21) |
2006 |
Public places |
Riyadh |
225 |
37.92 (7.89) |
Mothers |
Parents of children with Down syndrome |
Around two-thirds of the mothers breastfed their children and started wearing after 6-9 months of age |
|
Al-Hussyeen et al. (22) |
2006 |
Public places |
Riyadh |
225 |
7.24 (4.11) |
Children |
Children |
Satisfactory levels of dietary habits among the included families and occupation status were associated with it. |
|
Mohamed et al. (23) |
2013 |
Public places |
Riyadh |
221 |
- |
Children |
Children with DSS compared with their siblings |
36% of the Down syndrome children were bottle-fed while only 5.5% of their siblings were. Fruit, vegetables, meat, fast foods, and whole milk consumption were all significantly lower in the Down syndrome group than with their siblings |
|
Samarkandy et al. (24) |
2012 |
Public places |
Riyadh |
221 |
- |
Children |
Children with DSS compared with their siblings |
Fat, protein, riboflavin, retinol, calcium, and sodium, and potassium intake were significantly lower in the Down syndrome group than in the other group |
Risk of bias
The results of the risk of bias assessment are presented in Table 2. In brief, two articles were assessed as having good quality, while the other two had satisfactory results, indicating a low degree of bias among the included investigations.
|
Table 2. Quality assessment and domains of the modified Newcastle-Ottawa scale (mNOS) for cross-sectional studies. |
||||||||||
|
Author |
Year |
Selection |
Comparability |
Outcome |
Total score |
Quality |
||||
|
Representativeness of the Sample |
Sample size |
Non Respondents |
Ascertainment of the Exposure |
The Subjects in Different Outcome Groups are Comparable |
Assessment of outcome |
Statistical analysis |
||||
|
Al-Sarheed et al. (21) |
2006 |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
7 |
Good |
|
Al-Hussyeen et al. (22) |
2006 |
+ |
+ |
+ |
+ |
+ |
5 |
Satisfactory |
||
|
Samarkandy et al. (24) |
2012 |
+ |
+ |
+ |
+ |
++ |
+ |
+ |
8 |
Good |
|
Mohamed et al.(23) |
2013 |
+ |
+ |
+ |
+ |
+ |
+ |
6 |
Satisfactory |
|
Discussion
In the present systematic review, we have collected all the studies that were previously conducted in Saudi Arabia that discuss the feeding habits for children with Down syndrome, and the results of these studies are discussed in this section, together with comparative findings from other similar worldwide investigations for proper validation of our formulated evidence. In Saudi Arabia, we found four relevant investigations. Among these, Al-Sarheed et al. (21) reported that exclusive breastfeeding was introduced by around two-thirds of the included mothers, while the rest introduced formula-based regimens to their children with Down syndrome. More than 60% of the included mothers breastfed their children for more than 6 months, which gradually declined as children grew older. In addition, the authors reported that most of the included children (45.8%) were weaned at 6-9 months of age. No socio-economic characteristics were significantly associated with any of the feeding habits or the age when solid foods were introduced. There was a significant correlation between maintaining breastfeeding for 3-6 months and non-working and being literate. Mohamed et al. (23) also reported that around 36% of the children with Down syndrome were bottle-fed while only 5.5% of their siblings were bottle-fed during their infancy period. Moreover, they showed that around 50% of the children with Down syndrome were breastfed for at least six months during their infancy while only 36.5% of their siblings were. Hospital encouragement of breastfeeding was lower for children with Down syndrome than their siblings. Finally, solid food introduction was markedly more frequently delayed in the Down syndrome group. Fruit, vegetables, meat, fast foods, and whole milk consumption were all significantly lower in the Down syndrome group than with their siblings, while consuming skimmed or low-fat milk was significantly higher in children with Down syndrome. These findings were supported by another investigation by Samarkandy et al. (24) that assessed the nutritional status of children with Down syndrome and their siblings and found that no significant differences were found between the two groups in terms of caloric intake. However, fat, protein, riboflavin, retinol, calcium, and sodium, and potassium intake were significantly lower in the Down syndrome group than in the other group, while other minerals did not show any statistical significance between the two groups. Another investigation by Al-Hussyeen et al. (22) that aimed to investigate the dietary habits and oral hygiene practices among children with Down syndrome reported that 56% of the included mothers indicated that their children were frequently given sweets. Moreover, they reported that 56.2% of these mothers reported that they occasionally gave sweets to their children as a reward. The frequency of sweets consumption was significantly associated with the working status of the corresponding mothers, but neither the educational level, university education, or being illiterate were.
Many worldwide investigations were conducted to assess the frequency of breastfeeding and dietary practices among children with Down syndrome, and the estimated rates for feeding habits were variable across the different studies in the literature. In Italy (25), the rate regarding exclusive breastfeeding for children with Down syndrome was 43%, compared to 55% in Israel (6), to 48% in the Netherlands (8), and 63% in Mexico (26). This indicates that reported rates for the Saudi cohorts are among the highest globally, although not many studies were published across the Kingdom. It was also previously demonstrated the duration of breastfeeding lasted for a significantly longer period in the control group when compared to the Down syndrome group (25). Additionally, maternal depression, insufficient perceived milk, prematurity, suckling difficulties, and congenital malformations were all significantly reported factors that were associated with reduced breastfeeding practices (6, 21, 25, 27). The early termination of breastfeeding is also significantly associated with maternal depression and stress that usually results from the diagnosis of the syndrome in their children (21, 25). Therefore, professional healthcare advice and support should be offered to all mothers with children with Down syndrome to decide whether or not to stop breastfeeding and decide what is best for their children to enhance their outcomes.
Issues regarding swallowing and feeding are also common among children with Down syndrome, and although they were not reported in any of the included Saudi investigations, they were commonly reported among other global studies in the literature. It has been estimated that up 60% of children with Down syndrome have feeding difficulties (28, 29), up to 40% might require the installation of a nasogastric tube (6, 27, 30), and up to 5% might require gastrotomy (6, 27). Parenteral feeding habits are also important when studying the feeding habits and nutritional assessment in children with Down syndrome. For instance, a previous investigation showed that nutritional monitoring and feeding restrictions were more common among parents of overweight Down syndrome children than other parents of normal range weight Down syndrome children (31). A further report showed that 47% of parents of children with Down syndrome reported that their children continued to eat as long as the food was present before them (32). However, it should be noted that the evidence regarding this point is still poor, even within global settings, and therefore, further investigations are encouraged to enhance this point.
Our study is limited by the very small number of the included studies that were conducted in Saudi Arabia and the very low number of the included populations among them. Additionally, the heterogeneity among the included studies is also significant regarding the reported outcomes which made it hard to compare these outcomes among the included investigations. However, we performed a rapid review of the current literature as discussed above to elucidate our findings and compare them to the worldwide investigations.
Conclusion
Our results indicate that the rate of exclusive breastfeeding is relatively high among our population and it also lasts for an acceptable duration during infancy as compared to worldwide investigations. However, the evidence is still poor and it is hard to formulate a solid conclusion as a result of the small number of studies conducted across the Kingdom. Accordingly, further investigations are encouraged to strengthen the current evidence.
Declaration
Statement:
The authors declare no conflict of interest.
Funding:
None.
Ethical Consideration:
None applicable.
Data Availability:
All data is available withing the article.