Volume 4, Issue 11
November 2024
Oral Cancer Screening in Geriatrics: Importance, Tools, and Outcomes
Ahmed Fahad Althumairy, Jaber Mahdi Alyami, Abdullah Mahdi Alyami, Rakan Mohammed Al Abduljabbar, Norah Mufiz Alfawaz, Abdulrahman Hussain Khbrani
DOI: http://dx.doi.org/10.52533/JOHS.2024.41104
Keywords: Oral cancer screening, geriatrics, early detection, diagnostic tools, quality of life, healthcare management
Screening for oral cancer is crucial in the elderly population because the disease's risk rises with age. The importance of early detection and treatment of oral potentially malignant disorders (OPMDs) cannot be overstated, as they significantly impact morbidity, and healthcare costs. Various screening tools and techniques, including visual and physical examinations, biopsies, vital staining, brush biopsies, saliva analysis, and advanced imaging methods, play essential roles in early diagnosis. Each method has unique advantages and limitations, contributing to comprehensive patient assessment. The combination of these tools allows for more accurate and early detection, improving treatment outcomes and preserving function and quality of life. By integrating regular oral cancer screenings into routine healthcare for the elderly, healthcare providers can enhance proactive health management and reduce the public health burden of oral cancer. This review emphasizes the need for educating general practitioners on the risk factors, clinical presentations, and diagnostic techniques for effective oral cancer screening in geriatrics.
Introduction
Caring for elderly patients requires a deep understanding of the biology and neuropsychology of aging, the diseases, and conditions more common in elderly individuals, and how these factors affect function, impede patient goals, and lead to disability. The physical medicine and rehabilitation specialist is well-suited for geriatric care because physiatrists have experience working with interdisciplinary teams, treating patients with complex conditions, and are trained to focus on patients' goals and function (1).
Geriatric rehabilitation can be approached from a purely functional perspective, evaluating not only pathophysiology but also function and disability. For instance, tight hip extensors can hinder gait efficiency, preventing a person from walking quickly enough to cross the street while the traffic light signals "walk." However, aging with a disability presents a separate and more challenging process. A physiological insult and impairment sustained earlier in life may affect an individual's capacity to cope and compensate with age. Changes in health or psychosocial support systems over time can negatively impact mobility, self-care, and independence. Geriatric rehabilitation addresses problems that affect not only the individual patient but also society at large, with major economic ramifications when individuals can no longer care for themselves. Increased longevity and the aging global population will significantly impact society during the 21st century. The average life expectancy at age 65 is 15 to 20 years for the global population (1).
Oral potentially malignant disorders (OPMDs) refer to any oral mucosal abnormality that is associated with a statistically increased risk of developing oral cancer (2). The etiological factors for OPMDs are varied and include the use of toxic substances such as betel nut, alcohol abuse, or reverse smoking (3). Additionally, certain conditions like autoimmune disorders or sun exposure can also lead to OPMDs. Other contributing factors may include vitamin/mineral deficiencies, specific viruses, or genetic predisposition (4). The prevalence of some OPMDs is higher among middle-aged and older adults.
Oral leukoplakia is more frequently observed in men aged 40 and older (5), with an increased prevalence in both men and women over 70 (6). Oral erythroplakia has a higher prevalence in middle-aged and older adults, when reported (7). Proliferative Verrucous Leukoplakia (PVL) (8) and oral lichen planus (9) are more common in older women. Actinic keratosis is more prevalent in individuals aged 50 and above who have had prolonged sun exposure. Dyskeratosis congenita typically presents in individuals aged 5 to 12, but it is included in this review for completeness (3).
As people worldwide are living longer, early detection and treatment of OPMDs are essential to prevent morbidity. It is crucial to educate general practitioners about the risk factors, clinical presentation, differential diagnosis, and treatment of these disorders.
Methodology
This study is based on a comprehensive literature search conducted on 19 May 2024, in the Medline and Cochrane databases, utilizing the medical topic headings (MeSH) and a combination of all available related terms, according to the database. To prevent missing any research, a manual search for publications was conducted through Google Scholar, using the reference lists of the previously listed papers as a starting point. We looked for valuable information in papers that discussed oral cancer screening in geriatrics: importance, tools, and outcomes. There were no restrictions on date, language, participant age, or type of publication.
Discussion
The severity of the disease and the challenging therapies that frequently accompany it, which can cause severe functional impairment, psychological distress, deformity, and a reduced quality of life, may be minimized with early detection of oral malignancies. In the last 20 years, there has not been much advancement in the early detection of oral cancers (10). Nowadays, a considerable proportion of people receive a diagnosis after their disease gets to a more advanced stage. Dysplastic lesions, which are apparent precancerous indications, frequently lead to the development of oral squamous cell carcinoma (OSCC) (11).
Evaluation of the elderly patient
Medical history
When examining elderly patients, questions should be directed toward the patient rather than the caregiver or family member. While time management is important when dealing with complex problems, spending sufficient time, and showing patience will help develop the patient-physician relationship and improve care. The review of systems in geriatric patients may be complex if the patient has multiple system problems. Focusing on recent changes in constitutional symptoms—including fatigue, sleep, weight loss/appetite, pain, and falls—may be particularly informative (12). Fatigue has multiple causes and warrants a thorough evaluation. If sleep is impaired, the reason should be identified, whether it is due to pain, nocturia, or a mood disorder. Nocturia can result from the nighttime mobilization of peripheral edema, and urinary frequency, urgency, and subjective retention need to be identified and treated. Urinary incontinence should be addressed, as patients might be embarrassed to bring it up (1). Assessing nutrition is important; if it is inadequate, the reasons should be explored, such as financial issues, physical inability to get to supermarkets, difficulty carrying food items, or fear of lifting hot items while cooking. When pain is a symptom, history should specifically identify the sites and quality of the pain, as many older adults have multiple potential causes. Changes in bowel or bladder function should be assessed, as some elderly patients may assume new symptoms are merely a result of old age. Patients should be asked if they have fallen in the last 12 months and about the circumstances of the fall, as those who report a fall within the past year are at higher risk for future falls (13). Questions about specific activities of daily living (ADLs) are important, such as: Can you get in and out of the bathtub without assistance? and how often do you leave home? Additionally, assessing alcohol use is necessary, as it may contribute to nutritional deficiencies and falls. Age alone does not preclude the use of illicit drugs. The presence of informal support systems, such as neighbors who can help, should be noted. The history should also include a discussion of advanced directives, with the patient's goals and wishes prioritized in the treatment plan, as these may differ from those of the family and caregivers (1).
Medication
All medications should be reviewed, and medication reconciliation should be performed at each visit to identify potentially inappropriate medications that may increase the risk of adverse drug-related events in elderly patients (14). This is particularly important if the patient is experiencing new or worsening symptoms. Common adverse effects of medications include sedation, confusion, visual problems, insomnia, dizziness, headaches, fatigue, muscle pain, or cramps. These symptoms, though not always considered serious, can affect function and quality of life, and predispose patients to falls and other problems. Special attention should be paid to medications with central nervous system (CNS) activity, such as antidepressants, benzodiazepines, and those with anticholinergic effects. The necessity and efficacy of each medication should be evaluated, considering renal clearance and potential drug-drug interactions. A risk-benefit assessment should be performed for potentially inappropriate prescriptions, with alternatives considered. Patients should also be asked about nonprescription medications, supplements, or vitamins they may be taking (1).
Screening tools
Screening is looking for cancer before a person has any symptoms. This can help find cancer at an early stage. When abnormal tissue or cancer is found early, it may be easier to treat. By the time symptoms appear, cancer may have begun to spread (15).
Visual and physical examination
Visual and physical examination is a fundamental tool in oral cancer screening for geriatrics, involving a thorough inspection of the oral cavity, including lips, gums, tongue, and throat, along with palpation to feel for lumps, thickened areas, or other abnormalities in the oral tissues. This method is essential for early detection and effective management of potential oral health issues (15).
Biopsy and histopathological examination
A biopsy should include both suspicious and unaffected tissue, ensuring ample sampling for a conclusive diagnosis. Dysplasia is more likely in red regions, so these areas should be included. Most biopsy sites heal quickly, within a few days. To avoid potential setbacks from unfavorable pathology reports, some practitioners perform multiple biopsies initially. When doing excisional biopsies, care should be taken because they might not remove enough margins in cases of malignancy, which would reduce options for additional therapy. Diagnosing carcinoma through histopathology involves identifying severe dysplasia and invasion of the lamina propria. Incisional biopsies can yield false negatives, and interpretations can vary (16).
Stains
Many attempts to identify potential dysplastic regions before biopsy have unfortunately not been completely reliable. However, these methods can still be helpful, particularly in cases characterized by extensive 'field change,' a phenomenon often observed in individuals at elevated risk for OSCC. Toluidine blue staining is a simple and cost-effective diagnostic technique that uses blue dye to highlight abnormal mucosal areas. To target nuclear material in malignant and potentially malignant lesions (PML), toluidine blue (TB) employs a basic metachromatic nuclear dye while preserving healthy mucosa. The TB staining process involves several steps (Table 1) (11).
The preoperative value of TB staining is significant. Its efficacy for detecting OSCC was demonstrated in a case study where pre-malignant or malignant cells were found more than 1 cm away from the visible lesion. This discovery led to a resection that might not have been considered based solely on conventional oral examination (COE) (18).
TB staining can detect OPMDs with an elevated risk and poor prognosis (17).
|
Table 1. TB staining process (11) |
|
|
Step |
Description |
|
1 |
Rinse mouth with 1% acetic acid solution for 20 seconds. |
|
2 |
Rinse mouth with water for 20 seconds (repeated twice). |
|
3 |
Rinse mouth with 1% toluidine blue solution (5-10 cc). |
|
4 |
Rinse mouth with 1% acetic acid solution again. |
Brush biopsy
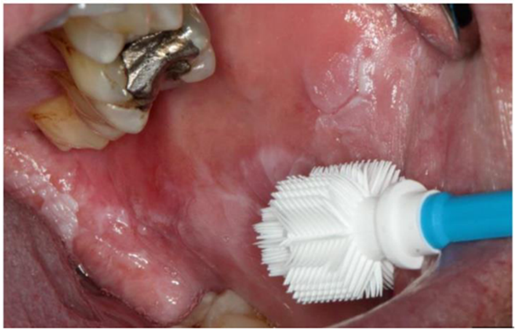
Utilising a tiny nylon brush, the brush biopsy gathers cytology specimens that are subsequently scanned and analysed by a computer utilising Oral CDx (Figure 1). This method detects and displays cells for pathologist assessment. A written report and cell printout are given if the condition is malignant. A standard biopsy should be ordered if the results are positive. Potential false negatives have given rise to debate, yet the approach is still useful (11).

Figure 1: The Orcellex brush, a cell collector, is positioned in front of a leukoplakia on the buccal mucosa (11).
Saliva analysis
Saliva-based oral cancer diagnostics offer significant potential for early detection of oral squamous cell carcinoma (OSCC). Exfoliative cell samples have been used to detect genetic and microsatellite alterations in high-risk patients. The concept of a saliva test is particularly appealing, with hypermethylation patterns of tumor suppressor genes and stable mRNAs like β-actin and interleukin-8 serving as indicators. Studies have shown that specific mRNA signatures in saliva are present at higher levels in OSCC patients, achieving an accuracy rate of about 85%. Four key salivary mRNAs have demonstrated 91% sensitivity and specificity for OSCC detection. Additionally, elevated levels of soluble CD44 and specific bacterial counts in saliva have been associated with OSCC. Despite the promise, concerns about false negatives remain, and large-scale multicentred studies are needed to verify the reliability of these saliva-based tests. Nevertheless, these advancements represent a significant step forward in non-invasive cancer diagnostics (19). Saliva can include serum proteins and nucleic acids through various pathways (Table 2) (11).
Laser
Laser Capture Microdissection (LCM) is an advanced technique used in the screening and study of oral cancers. This method allows for the precise isolation of specific cells from a heterogeneous tissue sample, enabling detailed molecular analysis. LCM is particularly valuable in oral cancer research because it can target dysplastic or malignant cells within the complex architecture of the oral epithelium, providing insights into the genetic and molecular alterations associated with cancer progression (11).
In oral cancer screening, LCM is used to analyze genetic mutations, epigenetic changes, and protein expression profiles that indicate malignancy. This technique enhances the accuracy of diagnostic tests by ensuring that only the relevant cells are studied, thereby reducing the background noise from non-cancerous cells (20).
|
Table 2. Serum proteins and nucleic acids may be in saliva (11) |
|
|
Aspect |
Description |
|
Serum Proteins and Nucleic Acids |
These substances can enter saliva via acinar cell transport, passive diffusion, crevicular fluid outflow, or ultrafiltration through tight junctions. |
|
Cell-free RNA Molecules |
Saliva contains both intact and fragmented cell-free RNA molecules. |
|
microRNAs |
These small RNA molecules (18 to 24 nucleotides in length) found in saliva influence transcriptional processes. |
|
RNA Stability |
Despite the presence of various RNAses in saliva, these molecules are not completely degraded. |
|
mRNA |
mRNA in saliva is significant in forensic medicine for detecting mRNA markers to diagnose primary Sjögren’s syndrome, identify body fluids, and study sleep drive. |
Furthermore, LCM's ability to maintain the integrity of the captured cells facilitates downstream applications such as DNA, RNA, and protein extraction, allowing comprehensive multi-omics approaches to understand oral cancer biology. This precision and versatility make LCM a powerful tool in the fight against oral cancers, contributing to improved diagnostic accuracy and better patient outcomes (21).
Optical Coherence Tomography
Optical Coherence Tomography (OCT) generates high-resolution cross-sectional images of tissues, like epithelial layers and basement membranes, like ultrasound. Utilizing infrared light, OCT can penetrate up to approximately 2 mm, making it suitable for monitoring oral dysplasia and early detection of oral cancer. With a resolution of about 10 μm, OCT outperforms other imaging methods like MRI, CT scans, and ultrasound. However, it often lacks sufficient contrast, particularly when differentiating between neoplastic and normal tissues. To address this, a multimodal approach combining microneedles and ultrasound has been used to deliver gold nanoparticles (Au NPs), enhancing OCT penetration depth, and increasing contrast levels by approximately 150% for detecting oral carcinogenesis. Additionally, photoacoustic imaging, a novel optical diagnostic technique, uses brief laser pulses to induce ultrasound signals from tissues, resulting in temporary thermoelastic expansions due to optical absorption. An ultrasound transducer detects these photoacoustic waves, translating them into images based on their timing. This method offers excellent spatial resolution for describing tissue architecture and is particularly useful for assessing lymph nodes following major surgery (11).
Conclusion
Oral cancer screening in geriatrics is vital due to the elevated risk and improved outcomes associated with early detection. Utilizing a combination of visual exams, adjunctive tools, and advanced diagnostics can enhance early detection rates, improve treatment outcomes, and preserve the quality of life in older adults. Integrating regular oral cancer screenings into routine healthcare for geriatrics is essential for proactive health management and reducing the public health burden of oral cancer.
Disclosure
Conflict of interest
There is no conflict of interest.
Statement
No financial or personal relationship
Funding
No funding
Ethical Consideration
Not applicable.
Data availability
Data that supports the findings of this study are embedded within the manuscript which is based on a comprehensive literature search conducted in May 2024, in the Medline and Cochrane databases.
Author Contribution
The Authors contributed to conceptualizing, data drafting, collection and final writing of the manuscript.