Volume 2, Issue 1
January 2022
Readiness to Receive COVID-19 Vaccine of General Population, Healthcare Workers and Medical Students in Jeddah Saudi Arabia
Reem Alnemari, Omar Aljohani, Abdulrahman Alnemari, Mishal Awaji, Abdullah Alali, Mohammed Almarshoud, Khalid Alzahrani, Wajd Abualamah
DOI: http://dx.doi.org/10.52533/JOHS.2021.2104
Keywords: COVID-19 Infection, COVID-19 Vaccination, Vaccine Acceptance, Readiness, Medical students, Healthcare workers, Saudi Arabia
Background: The COVID-19 pandemic has affected the healthcare system, economy, and social life worldwide. Much effort has been made to develop a COVID-19 vaccine to control the pandemic. Therefore, it is crucial to understand the factors that cause uncertainty about vaccination against COVID-19. The study aims to assess readiness to receive COVID-19 vaccination among the general population, healthcare workers, and medical students in Jeddah, Saudi Arabia.
Methods: This cross-sectional study was conducted in King Abdulaziz Hospital, East Jeddah General Hospital, and King Fahad General Hospital in Jeddah, Saudi Arabia in June–August 2021. An online self-administered questionnaire in Google Form was distributed among healthcare workers and hospital visitors. Participants were selected via a convenient non-probability sampling technique. Data analysis was performed using SPSS.
Results: A total of 300 participants were included in this study. More than half of the respondents were aged 18 to 25 years. Although almost 14% of our participants were not vaccinated, 82.9% of them were willing to get vaccinated. Approximately half of the respondents thought that COVID-19 vaccine is protective, and 18.7% thought it is not protective; 39% of the respondents were afraid of the side effects of the vaccine. Medical professionals and social media were the primary sources of information. The Pfizer/BioNTech vaccine was found to be preferred by 81% of the respondents. A significant difference in readiness was observed between different nationalities (P=0.018): Saudi nationals (86.8%) showed a higher level of readiness to get vaccinated than non-Saudi nationals (33.3%).
Conclusion: Overall, a multifaceted approach is needed to increase vaccine awareness. Therefore, further research is recommended to consider the scope of readiness for COVID19 vaccination to build confidence in the COVID-19 vaccine effort.
Background
Clusters of cases of pneumonia of unknown origin were reported on December 31, 2019 in the Wuhan City of China (1). Soon after, other countries started reporting the emergence of the same cases, with the first case in the USA appearing on January 20, 2020 (2). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causal organism for the COVID-19 infection, spread quickly and led to a global pandemic and public health crisis on an unimaginable level. There have been 174 million confirmed cases and 3 million deaths due to this disease till June 2021, as reported by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) (3). The first case of COVID-19 in Saudi Arabia was reported on March 2, 2020 (4). As of June 10, 2021, 459,968 confirmed cases and 7,488 deaths have been reported in Saudi Arabia by the World Health Organization (WHO) (5). SARS-CoV-2 is believed to spread primarily through airborne respiratory droplets from person to person when a person infected with this virus either talks, sneezes, or coughs (6,7). In addition to spreading from symptomatic patients, this virus can also transmit from asymptomatic patients before the onset of symptoms (8). Propagation is the way through which a virus transmits, and like most viruses, the propagation of SARS-CoV-2 can be inhibited through preventive measures. At present, there are no drugs or effective treatments available for COVID-19. Nevertheless, much emphasis is given to the importance of vaccination to combat the COVID-19 pandemic (9,10). Pharmaceutical companies, research institutions, and government organizations worldwide have come together to accelerate the process of vaccination against COVID-19 in the general public by hastening the efforts in the research, preparation, development, manufacturing, and logistics of vaccines (10,11).
Evidence suggests that the most effective method for controlling and preventing the spread infectious diseases is vaccination (12). Therefore, vaccination is considered the most reliable way to prevent and contain COVID-19 (13). Still, the effectiveness of vaccines in controlling and preventing COVID-19 depends on the population coverage. The protection of the vaccinated population is ensured through an adequate uptake of the vaccine. This will lead to the formation of herd immunity, which can eventually stop the pandemic (14). However, evidence suggests that hesitancy and reluctance exist among the populace because of complex influences and believes (12,15–20). In 2019, the WHO listed vaccine hesitancy as the number one reason for global health threats (21). The decision of a person to get themselves and their families vaccinated is greatly influenced by several factors, such as concerns regarding safety, perceived effectiveness, adverse reactions, and personal experiences (16).
Barriers to attaining herd immunity that is effective against infectious diseases of highly transmissible nature include refusal and delay of vaccination, despite vaccines being available (17,22). Moreover, when the data related to the safety and efficacy of a new vaccine are insufficient, the general population becomes reluctant to receive it (23). Although efforts are being made to accelerate the process of vaccine development, a decline in intent among the public in the USA was observed by a recent study. It was reported that the intent to be vaccinated against COVID-19 decreased from 72% in May 2020 to 51% in September 2020 (24).
The world has evolved after the COVID-19 pandemic. This pandemic has also prompted people to pursue solutions for its control and prevention, including safe and effective vaccines (25). Vaccine manufacturers have successfully concluded phase 3 clinical trials by the end of 2020, giving hope to the world that this pandemic could be ended quickly. A promise that life will return to normal has also been established. This increases the importance of evaluating the attitude of the public, including healthcare workers and medical students, towards vaccination (26). The factors influencing vaccine hesitancy can be identified easily. This will help recognize the different factors affecting the ability of the public to adopt healthy practices (27). Wang et al. conducted a population-based study in China to assess the public’s willingness and hesitancy towards vaccination against COVID-19. According to the results, 69% of the population showed trust in vaccines, and 67.1% of the population was willing to get vaccinated, whereas 9% refused to get vaccinated (28). Marques et al. conducted a study in Ohio City to examine the acceptance of parents towards an on-coming COVID-19 vaccine. Out of the total participants, 39.2% of caregivers or parents refused to vaccinate their children, whereas 27.8% of parents or caregivers agreed to vaccinate their child; 52.2% said they would only do this if their doctor approved it (29). Multiple studies have been conducted to assess the readiness of healthcare workers for COVID-19 vaccination. For example, a study showed a lower degree of trust in COVID-19 vaccines among healthcare workers who were not dealing with COVID-19 patients. In addition, a higher degree of hesitance towards COVID-19 vaccination was found in nurses than in physicians (30). Chew et al. conducted a study on healthcare workers in the Asia Pacific region, including China, India, Vietnam, Singapore, Bhutan, and Indonesia, to examine willingness to receive vaccination against COVID-19; 95% of the participants showed willingness to be vaccinated against COVID-19 (31). Manning et al. evaluated the readiness of nursing faculty members and students in the US for COVID-19 vaccination; 60% of faculty showed intention to receive the vaccination, but only 45% of students and adjunct faculty members showed willingness for vaccination against COVID-19 (32). In another study conducted in Greece, 51.1% of healthcare workers showed an intention to be vaccinated against COVID-19; however, 36.2% of them showed a concern for the safety of the vaccine (33). A cross-sectional study was conducted in Jordan on students aged 18 or older to evaluate the acceptance of COVID-19 vaccination in university students. The study found low acceptance among students: 34.9% of students said no to vaccination, and 25.5% said that they would probably get vaccinated. Male students and students of a health school also showed a high acceptance rate (42.1% and 43.5%, respectively) (34). Similar results were also reported by another study conducted in Kuwait, Jordan, and Saudi Arabia (35). Qunaibi et al. conducted a study on Arab healthcare workers residing in or outside Arab countries to assess their rate of acceptance towards COVID-19 vaccination; the results showed a low acceptance rate for COVID-19 vaccination among Arab healthcare workers (35). However, although large-scale studies to evaluate readiness for COVID-19 vaccination have been conducted in Arab countries, our literature search failed to find any study mainly focusing on the readiness of the Saudi public for Covid-19 vaccination. Therefore, the aim of the present study was to assess the readiness of the general public, healthcare workers, and medical students in Jeddah, Saudi Arabia to receive COVID-19 vaccination. The second objective was to explore the relationship between the level of readiness and different socio-demographic factors.
Methodology
Study setting
A cross-sectional study was conducted in King Abdulaziz Hospital, East Jeddah General Hospital, and King Fahad General Hospital in Jeddah, Saudi Arabia in June–August 2021. A convenient non-probability sampling technique was used to collect data from participants recruited from these hospitals. The inclusion criteria were any adult of both genders and any nationality aged >18 years who were healthcare workers or hospital visitors in Jeddah, Saudi Arabia, agreed to participate in the study, and had a social media account. Those who did not meet the inclusion criteria or refused to share information were excluded from the study.
Data collection tool
The sample size was calculated using the EPI info program based on a 95% confidence interval, 5% margin of error, and the total population of Jeddah, Saudi Arabia. The estimated sample size was 384, which was then adjusted to 422 to compensate for 10% non-response rate. The study was conducted using an online self-administered questionnaire via Google Form. The generated link was randomly shared on social media (i.e., Facebook, WhatsApp, Telegram, and Twitter). The aim of the study was clearly explained in the interface. A validated questionnaire was used based on previous studies. The questionnaire contains questions about the socio-demographic characteristics of the participants, such as age group, sex, nationality, profession, and residence. The questionnaire also includes questions about readiness to receive COVID-19 vaccination. The questionnaire was pretested in a pilot study over a sample of 20 participants whose results were not included in the present study. Some questions were modified accordingly to ensure clarity and easy understanding of the questions.
Statistical analysis
Data were coded, entered, and analysed using Statistical Package for Social Science (SPSS) version 23. Qualitative data were expressed in numbers (No.) and percentages (%). Chi-square (χ2) test was used to compare qualitative data between two groups.
Results
Socio-demographic data of the study respondents
A total of 300 respondents were included in the study, most of whom were females (56.7%), and 130 (43.3%) were males. More than half of the respondents were in the age group of 18 to 25 years, and only 21 (7%) were in the age group of 46 to 65 years. The majority of the respondents were of Saudi nationality (94.7%). Regarding the education level of the respondents, most of them (72.7%) had completed their Bachelor’s degree, and 20.3% had completed secondary school. Most of the respondents were single during the time of this study (69.3%), whereas the others were: married (28.7%), divorced (1.7%), or widowed (0.3%). Furthermore, most of the respondents (32.7%) were medical students, and 67 (22.3%) were healthcare workers. Regarding the average monthly income, approximately one-third (30%) of the respondents had a monthly income of more than 20,000 SAR. The characteristics of the participants are presented in (Table 1).
Table 1: Socio-demographic data of the study respondents (n=300)
|
Variable |
Category |
Frequency |
Percent |
|
Gender |
Male |
130 |
43.3% |
|
Female |
170 |
56.7% |
|
|
Age (years) |
18-25 |
173 |
57.7% |
|
26-35 |
77 |
25.7% |
|
|
36-45 |
29 |
9.7% |
|
|
46-65 |
21 |
7% |
|
|
★ 66 |
0 |
0 |
|
|
Nationality |
Saudi |
284 |
94.7% |
|
Non-Saudi |
16 |
5.3% |
|
|
Level of education |
Primary |
1 |
0.3% |
|
Intermediate |
2 |
0.7% |
|
|
Secondary |
61 |
20.3% |
|
|
Bachelor’s degree |
218 |
72.7% |
|
|
Master’s degree/PhD |
18 |
6% |
|
|
Marital status |
Single |
208 |
69.3% |
|
Married |
86 |
28.7% |
|
|
Divorced |
5 |
1.7% |
|
|
Widowed |
1 |
0.3% |
|
|
Occupational status |
Educational sector |
29 |
9.7% |
|
Healthcare worker |
67 |
22.3% |
|
|
Medical student |
98 |
32.7% |
|
|
Military sector |
8 |
2.7% |
|
|
Private business |
10 |
3.3% |
|
|
Retired |
6 |
2% |
|
|
Others |
82 |
27.3% |
|
|
Average monthly income (SAR) |
< 10,000 |
86 |
28.7% |
|
10,000–15,000 |
68 |
22.7% |
|
|
16,000–20,000 |
56 |
18.7% |
|
|
> 20,000 |
90 |
30% |
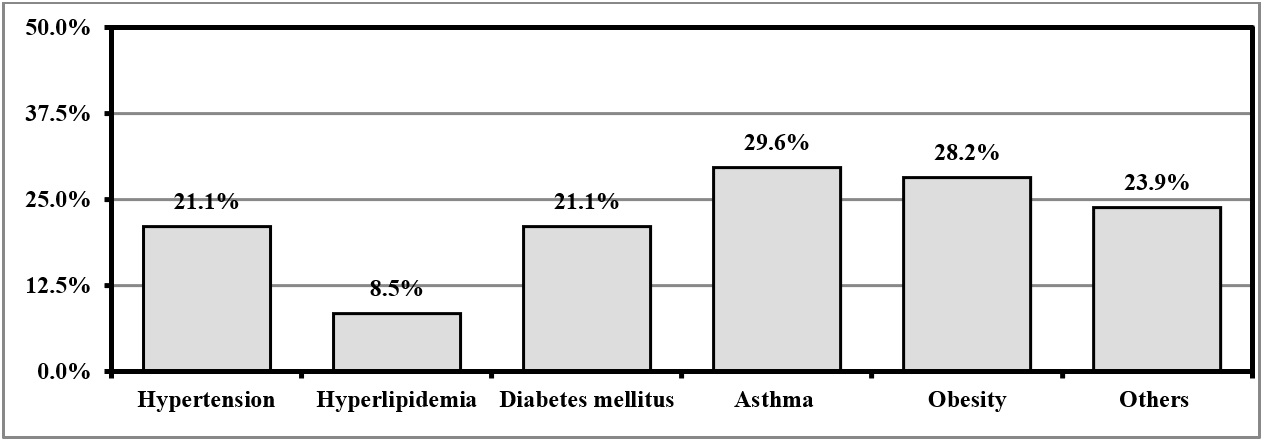
Regarding history of chronic illnesses, 71 (23.7%) of the respondents had chronic diseases, whereas 229 (76.3%) had no medical conditions. Out of 71 respondents, 21 (29.6%) had asthma, 20 (28.2%) had morbid obesity, 15 (21.1%) had diabetes mellitus, 15 (21.1%) had hypertension, 6 (8.5%) had hyperlipidaemia, and 17 (23.9%) had other illnesses (Figure 1).

Figure 1: Frequency of medical conditions among participants (n=71)
History of COVID-19 infection and thoughts about vaccines
Regarding history of COVID-19 infection, 67 (22.3%) of the participants had been diagnosed with COVID-19, with 64 (95.5%) of the infected respondent requiring home isolation and 3 (4.5%) requiring hospital admission. Approximately 168 (56%) of the respondents had a household or close family member who suffered from COVID-19, of which 141 (83.9%) required home isolation, 17 (10.1%) required hospital admission, and 7 (4.2%) required ICU admission. In addition, 28 (9.3%) of the respondents had a household or close family member who died due to COVID-19. Regarding vaccination, 259 (86.3%) of the respondents had received COVID-19 vaccination, whereas 41 (13.7%) had not, of which 34 (82.9%) expressed willingness to get vaccinated, whereas 7 (17.1%) said no when asked about their willingness for vaccination.
Approximately 206 (68.7%) of respondents thought vaccines protect against infectious diseases, and 120 (40%) thought vaccines have health-related risks. Moreover, 128 (42.7%) of respondents thought that the spread of COVID-19 will be mitigated when a large percentage of the population becomes infected. Approximately 129 (43%) of respondents thought that it is very likely to have other waves of COVID-19 outbreaks in their country, and 169 (56.3%) thought that vaccination should be mandatory. The COVID-19 infection history of the participants and their thoughts about vaccines are presented in Table 2.
Table 2: History of COVID-19 infection and thoughts about vaccines (n=300)
|
Yes |
No |
||
|
Have you ever suffered from COVID-19★ |
67 (22.3%) |
233 (77.7%) |
|
|
Has any of your household or close family member suffered from COVID-19★ |
168 (56%) |
132 (44%) |
|
|
Has any member of your household or close family died due to COVID-19★ |
28 (9.3%) |
272 (90.7%) |
|
|
Have you received the COVID-19 vaccine? |
259 (86.3%) |
41 (13.7%) |
|
|
Yes |
No |
Not sure |
|
|
Do you think vaccines protect against infectious diseases? |
206 (68.7%) |
22 (7.3%) |
72 (24%) |
|
Do you think vaccines have health-related risks? |
120 (40%) |
66 (22%) |
114 (38%) |
|
Do you think that the spread of COVID-19 will be mitigated when a large percentage of the population has become infected? |
128 (42.7%) |
74 (24.7%) |
98 (32.7%) |
|
Do you think it is very likely to have other waves of COVID-19 outbreaks in our country? |
129 (43%) |
62 (20.7%) |
109 (36.3%) |
|
Do you think that vaccination should be mandatory? |
169 (56.3%) |
91 (30.3%) |
40 (13.3%) |
Participants were asked if their point of view on vaccination, in general, was changed recently. Most of them (51%) said no, whereas 123 (41%) said that their opinion was positively changed, and only 24 (8%) said that their opinion was changed in a negative way (Figure 2).

Figure 2: Changes in the point of view of the respondents on vaccination (n=300)
Thoughts of the respondents about COVID-19 vaccines
Regarding the thoughts of the respondents about COVID-19 vaccines, most of them (52%) thought that vaccines are protective, and half of them encouraged family members over the age of 50 to get vaccinated, whereas 117 (39%) of the respondents were afraid of side effects of the vaccine. In addition, 103 (34.3%) respondents encouraged family members aged 12-18 to get vaccinated. More information on the respondents’ thoughts is presented in Table 3.
Table 3: What are your thoughts on COVID-19 vaccines? (n=300)
|
Thoughts |
N (%) |
|
I am afraid of the side effects |
117 (39%) |
|
I do not trust the vaccines |
32 (10.7%) |
|
I think that they are protective |
156 (52%) |
|
I do not think that they will protect me |
56 (18.7%) |
|
I do not think that COVID-19 is a threat against my health |
35 (11.7%) |
|
I encourage my family members aged ★ 12 to get vaccinated |
56 (18.7%) |
|
I encourage my family members aged12-18 to get vaccinated |
103 (34.3%) |
|
I encourage my family members over the age of 50 to get vaccinated |
150 (50%) |
|
I am afraid of taking the vaccine during my pregnancy |
53 (17.7%) |
|
I favour natural or alternative ways of healing |
22 (7.3%) |
|
I am against all kinds of vaccination |
6 (2%) |
Participants were asked about their sources of information related to vaccination. Medical literature was the most frequently reported source (51.7%), followed by social media (50%) and healthcare providers (26%). Other reported sources of information are shown in Figure 3.
Regarding vaccine preference, most respondents (81%) prefer the Pfizer/BioNTech vaccine, and 38 (12.7%) prefer the Oxford/AstraZeneca vaccine. The answers of the respondents are summarized in Figure 4.

Figure 3: Sources of information related to vaccination (n=300)

Figure 4: Which vaccine would you prefer? (n=300)
Factors associated with readiness for COVID-19 vaccination
To investigate the effect of socio-demographic factors on the readiness of the studied population to receive COVID-19 vaccination, we identified the significant factors using chi-square test. A significant association (P < 0.05) was found with nationality (P = 0.018); more Saudi nationals (86.8%) were ready for vaccination than non-Saudi nationals (33.3%). The other studied socio-demographic factors did not reach the significance level of P < 0.05. More information on the factors associated with readiness for COVID-19 vaccination is provided in Table 4.
Table 4: Factors associated with readiness for COVID-19 vaccination
|
Variable |
Category |
Willing to receive COVID-19 vaccination |
P value |
|
|
Yes N (%) |
No N (%) |
|||
|
Gender |
Male |
15 (88.2%) |
2 (11.8%) |
0.447 |
|
Female |
19 (79.2%) |
5 (20.8%) |
||
|
Age (years) |
18-25 |
18 (81.8%) |
4 (18.2%) |
0.744 |
|
26-35 |
6 (75%) |
2 (25%) |
||
|
36-45 |
6 (85.7%) |
1 (14.3%) |
||
|
46-65 |
4 (100%) |
0 (0%) |
||
|
Nationality |
Saudi |
33 (86.8%) |
5 (13.2%) |
0.018 |
|
Non-Saudi |
1 (33.3%) |
2 (66.7%) |
||
|
Level of education |
Primary |
1 (100%) |
0 (0%) |
0.879 |
|
Intermediate |
1 (100%) |
0 (0%) |
||
|
Secondary |
5 (71.4%) |
2 (28.6%) |
||
|
Bachelor’s degree |
23 (85.2%) |
4 (14.8%) |
||
|
Master’s degree/PhD |
4 (80%) |
1 (20%) |
||
|
Marital status |
Single |
23 (85.2%) |
4 (14.8%) |
0.677 |
|
Married |
8 (72.7%) |
3 (27.3%) |
||
|
Divorced |
2 (100%) |
0 (0%) |
||
|
Widowed |
1 (100%) |
0 (0%) |
||
|
Occupational status |
Educational sector |
4 (100%) |
0 (0%) |
0.693 |
|
Healthcare worker |
10 (83.3%) |
2 (16.7%) |
||
|
Medical student |
8 (88.9%) |
1 (11.1%) |
||
|
Private business |
1 (100%) |
0 (0%) |
||
|
Others |
11 (73.3%) |
4 (26.7%) |
||
|
Average monthly income (SAR) |
< 10,000 |
7 (63.6%) |
4 (36.4%) |
0.214 |
|
10,000–15,000 |
14 (87.5%) |
2 (12.5%) |
||
|
16,000–20,000 |
7 (87.5%) |
1 (12.5%) |
||
|
> 20,000 |
6 (100%) |
0 (0%) |
||
|
Having medical condition |
Yes |
13 (86.7%) |
2 (13.3%) |
0.629 |
|
No |
21 (80.8%) |
5 (19.2%) |
||
Discussion
In this cross-sectional study, we assessed the readiness for COVID-19 vaccination and explored the relationship between readiness level and different socio-demographic factors among the general population, healthcare workers, and medical students in Jeddah, Saudi Arabia. Readiness for vaccination can significantly control the COVID-19 pandemic. However, vaccine production is challenging, and convincing people to get vaccinated is also a major issue.
Our findings revealed that 82.9% of our participants were willing to receive vaccination, and 86.3% of them were already vaccinated. This high vaccination and acceptance rate is consistent with that in other studies in Saudi Arabia, which reported a rate between 60–80% (37-39). Furthermore, it agrees with a study conducted in Middle East countries, which stated that the public of Iraq and Saudi Arabia were significantly more likely to accept the vaccine than the people of other countries studied (40). Different rates of readiness for vaccination, either high or low, have been reported. An earlier study in Jordan reported that only 37.4% of healthcare workers were willing to get vaccinated when the vaccines would be available (41). Readiness to receive any vaccine varies from one population to another, and readiness to receive the COVID-19 vaccine can change significantly over time and experience with actual vaccination.
The current study showed that 39% of participants were at some point concerned about the safety of vaccines, as evidenced by concerns about the associated side effects; this is consistent with a Jordanian study in which half of the participants were concerned about the side effects of COVID-19 vaccines (41). However, half of the respondents encouraged their family members over the age of 50 to get vaccinated. In addition, more than half of the participants in the current study stated that receiving the vaccine is essential to protect against COVID-19.
During the COVID-19 pandemic, people have used various information sources to gain health knowledge and information about the disease. In our study, participants identified health care providers and social media as the most trusted sources of COVID-19 information; this is in line with another study conducted in Saudi Arabia (39). These results highlight the need for news about the COVID-19 vaccine to be communicated primarily by health authorities and social media campaigns. Therefore, understanding the sources people trust most to gain information about the COVID-19 vaccine is essential for future national vaccination campaigns. The Pfizer/BioNTech vaccine was found to be preferred by 81% of acceptors. Significant differences in readiness for vaccination were observed between nationalities (P = 0.018), with Saudi nationals (86.8%) having a higher level of vaccine readiness than non-Saudi nationals (33.3%).
More research on vaccination awareness and readiness is required to elucidate the variables contributing to the acceptance or rejection of each type of vaccine, depending on the different development platforms used. This understanding will help policymakers to develop appropriate teaching materials to build confidence in various vaccine platforms. A policy statement that supports the COVID-19 vaccine and plays a vital role in calming, educating, and encouraging the public about the safety and efficacy is of great value. Our research, however, had some limitations. The survey was distributed online rather than physically, which can lead to selection bias because our survey may have missed a response from a particular population segment. Future studies using mixed-method studies with qualitative and quantitative approaches are recommended to obtain the complete picture of the readiness of the public of Saudi Arabia to receive COVID-19 vaccination.
Conclusion
This study generally reflected a high willingness of the people of Saudi Arabia to receive the COVID-19 vaccine. In addition, Saudi nationals were more ready to receive the vaccine than non-Saudi nationals. The most commonly reported sources of information were medical professionals and social media. These findings may be used for communication coordination and advertising campaigns in the future to increase vaccine uptake and awareness.
Disclosure
Statement
The authors declare that they have no conflict of interest
Funding
The study did not receive any funding.
Ethical considerations
The study was approved by the Institutional Review Board of the General Directorate of Research and Studies, Ministry of Health, Jeddah, Saudi Arabia (IRB Registration Number KACST, KSA, H-02-J-002). All participants were volunteers and asked to do their best. All data were kept confidential and used only for research purposes.
Data Availability
All data is found within the manuscript
Authors’ Contributions
Reem Alnemari conceptualized and designed the study, critically revised the manuscript for key intellectual content, and approved the final version to be submitted. Omar Aljohani and Abdulrahman Alnemari carried out the literature review, contributed to the study design and methodology, and drafted the manuscript. Mishal Awaji and Abdullah Alali were responsible for data acquisition, analysis, and interpretation. Mohammed Almarshoud and Khalid Alzahrani were responsible for statistical analysis, IRB approval, and manuscript publication. Wajd Abualamah was responsible for criticizing the article for important intellectual content and gave the final approval of the version to be submitted.